PATIENTS AND CAREGIVERS DISCUSS THE PHYSICIAN DISCUSSION
-
drsclafani

- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
PATIENTS AND CAREGIVERS DISCUSS THE PHYSICIAN DISCUSSION
I desire that patients learn from a healthy debate among physicians. Interjection by patients may inhibit this. That is why i am proposing a separate thread for discussion of what transpires in a dialogue between physicians. Not wanting to in any way inhibit patients who have driven this discussion with patients and physicians i thought this would allow all to lurk or be heard.
the learning curve
Dr. Sclafani,
As more doctors start doing treatment for CCSVI, patients are understandably concerned about their competence. The doctors who have led the pursuit of CCSVI treatment have discussed how doing this kind of venogram has yielded unexpected findings, required innovations in treatment and the development of new tools (like stents, etc.).
I spoke recently to a doctor who has been an IR for a couple of decades. He was very excited about doing his first CCSVI treatment and seemed very comfortable with his skill set. As a patient, I'm looking for a way to balance his confidence based on his experience with the unknown factors that you and others have dealt with.
I assume one of the outcomes of the meetings planned for IRs this month and in March is to produce some sort of standardized treatment plan so new practitioners don't have to reinvent the wheel and study data can be gathered for future research.
Could you please put the learning curve into perspective for us? For example, is it like a car mechanic having to learn how to service a bus? There are some similarities, but "patient" is significantly different, he must use a larger garage and requires metric tools for treatment instead of his traditional ones.
Or is it more subtle, like the doctor has been baking cookies and now has to learn how to bake a cake? He still is using the same basic ingredients like the flour, sugar, mixing bowls and an oven, but now he has to learn to use a different kind of baking pan, using a different oven temperature and he has to learn about icing (meds).
How much/how long does this training take? Is it a couple of hours reviewing written material and viewing images of treatments? Or does it really take "co-piloting" to learn in the clinic while procedures are being done?
Gratefully,
Rosegirl
As more doctors start doing treatment for CCSVI, patients are understandably concerned about their competence. The doctors who have led the pursuit of CCSVI treatment have discussed how doing this kind of venogram has yielded unexpected findings, required innovations in treatment and the development of new tools (like stents, etc.).
I spoke recently to a doctor who has been an IR for a couple of decades. He was very excited about doing his first CCSVI treatment and seemed very comfortable with his skill set. As a patient, I'm looking for a way to balance his confidence based on his experience with the unknown factors that you and others have dealt with.
I assume one of the outcomes of the meetings planned for IRs this month and in March is to produce some sort of standardized treatment plan so new practitioners don't have to reinvent the wheel and study data can be gathered for future research.
Could you please put the learning curve into perspective for us? For example, is it like a car mechanic having to learn how to service a bus? There are some similarities, but "patient" is significantly different, he must use a larger garage and requires metric tools for treatment instead of his traditional ones.
Or is it more subtle, like the doctor has been baking cookies and now has to learn how to bake a cake? He still is using the same basic ingredients like the flour, sugar, mixing bowls and an oven, but now he has to learn to use a different kind of baking pan, using a different oven temperature and he has to learn about icing (meds).
How much/how long does this training take? Is it a couple of hours reviewing written material and viewing images of treatments? Or does it really take "co-piloting" to learn in the clinic while procedures are being done?
Gratefully,
Rosegirl
-
SaintLouis

- Family Elder
- Posts: 153
- Joined: Sun Dec 13, 2009 3:00 pm

-
DrCumming

- Family Elder
- Posts: 209
- Joined: Sat Dec 25, 2010 3:00 pm
- Location: Minneapolis, MN
- Contact:
Re: PATIENTS AND CAREGIVERS DISCUSS THE PHYSICIAN DISCUSSION
Sal, it would be great to have a way to post and discuss cases and management. A more modern day angio club for CCSVI.drsclafani wrote:I desire that patients learn from a healthy debate among physicians. Interjection by patients may inhibit this. That is why i am proposing a separate thread for discussion of what transpires in a dialogue between physicians. Not wanting to in any way inhibit patients who have driven this discussion with patients and physicians i thought this would allow all to lurk or be heard.

-
soapdiva884

- Family Elder
- Posts: 167
- Joined: Mon Apr 05, 2010 2:00 pm
- Contact:
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Case study #1
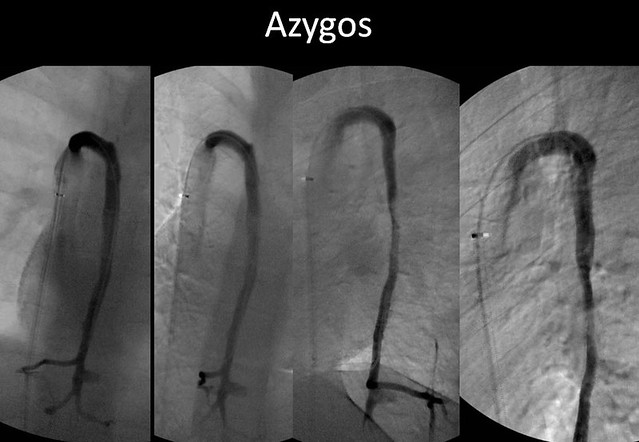
The patient is a 33 year old female with short term memory deficiencies, cognitive dysfunction, fatigue, headaches, and imbalance. She has numbness in both hands and the soles of both feet and temperature intolerance. Weakness is predominantly in the lower extremities. She has moderate spasticity, which is worse in the morning. She has co-morbidities of rheumatoid arthritis and multiple sclerosis.
Doppler and B-mode ultrasound of the neck in supine and erect positions and transcranial doppler of the deep cerebral veins was positive for more than one criteria and consistent with CCSVI.
Venography was performed via a left femoral approach.


 [/img]
[/img]
what is your interpretation?
What would be your next step?
Lurk away and learn
Doppler and B-mode ultrasound of the neck in supine and erect positions and transcranial doppler of the deep cerebral veins was positive for more than one criteria and consistent with CCSVI.
Venography was performed via a left femoral approach.
[/img]what is your interpretation?
What would be your next step?
Lurk away and learn
Re: Case study #1
Oh what fun.
The right jugular looks good except for I'd take a closer look in the proximal area with IVUS.
I find it hard to interpret azygous images, so I'd defer to my supervising physician on that (and really on all of this). But I would ask him about the apparent narrowing midway down and the apparent lack of issues up on the arch itself, since that is an area I'd expect to find something.
I would note that the ascending lumbar looks abnormal but would not treat in that area, the veins are too small and the association with CCSVI or MS too uncertain.
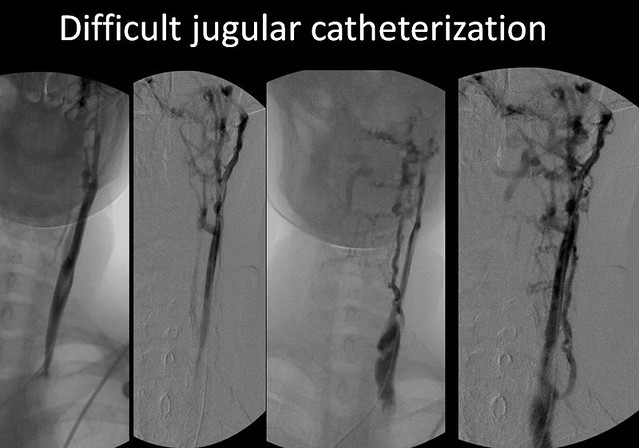
The left jugular, is that hypoplastic? Or is the technical term 'a mess.' I'd balloon starting from the bottom, going up, after double-checking drsclafani's thread for what balloon sizes and pressures he's used in hypoplastic veins and repeat ballooning or adjusting sizes and pressures on whatever waisting is found, but with the issues near the skull base I'd leave alone. I would not expect too good of results with that one but perhaps would be surprised.

(please note that I expect to be wrong and most definitely am not a doctor)
The right jugular looks good except for I'd take a closer look in the proximal area with IVUS.
I find it hard to interpret azygous images, so I'd defer to my supervising physician on that (and really on all of this). But I would ask him about the apparent narrowing midway down and the apparent lack of issues up on the arch itself, since that is an area I'd expect to find something.
I would note that the ascending lumbar looks abnormal but would not treat in that area, the veins are too small and the association with CCSVI or MS too uncertain.
The left jugular, is that hypoplastic? Or is the technical term 'a mess.' I'd balloon starting from the bottom, going up, after double-checking drsclafani's thread for what balloon sizes and pressures he's used in hypoplastic veins and repeat ballooning or adjusting sizes and pressures on whatever waisting is found, but with the issues near the skull base I'd leave alone. I would not expect too good of results with that one but perhaps would be surprised.
(please note that I expect to be wrong and most definitely am not a doctor)
-
civickiller
- Family Elder
- Posts: 558
- Joined: Thu Feb 04, 2010 3:00 pm
- Location: Hawaii
Right IJV looks fine. The left IJV looks like up at the base of the skull, by C1 there's stenosis resulting in spider veins and down the left IJV by shoulder height there appears to be spidering. normal i dont know.
For the Left IJV up by the base of the skull I would recommend upper cervical care to relieve any pressure the bones might be putting on the Left IJV. More down on the Left IJV shoulder height, I would check for CTOS, if its not CTOS then ballon to open it up
azygos appears normal but like cece said that narrowing midway down might cause some suspision, i would check it out just to make sure
For the Left IJV up by the base of the skull I would recommend upper cervical care to relieve any pressure the bones might be putting on the Left IJV. More down on the Left IJV shoulder height, I would check for CTOS, if its not CTOS then ballon to open it up
azygos appears normal but like cece said that narrowing midway down might cause some suspision, i would check it out just to make sure
-
- Similar Topics
- Replies
- Views
- Last post
-
- 1 Replies
- 11555 Views
-
Last post by ElliotB
-
- 0 Replies
- 1412 Views
-
Last post by NeusFunollet
-
- 0 Replies
- 861 Views
-
Last post by NeusFunollet
-
- 0 Replies
- 1429 Views
-
Last post by frodo
-
- 0 Replies
- 1460 Views
-
Last post by NHE
-
- 0 Replies
- 2233 Views
-
Last post by frodo
-
- 5 Replies
- 13283 Views
-
Last post by gibbledygook