Jasper9 wrote:But it's the science behind it (antigens, cytokines, FOXP3.....) that I'm finding hard to understand, and whether this science ties in at all with the science of HSCT.
I'll try to explain what I know about the science that I have surmised by reading a lot of research papers. I am not an expert, but I think I have a good grasp of what is involved.
First off there are two types of cells that are of concern when talking about adaptive immunity which is believed to be the mechanism involved in MS.
The first are effector T-cells which are otherwise known as helper T-cells. These cells do not directly cause cell damage, but rather recruit other cells such as machrphages to perform the attack on pathogens and cells that have been taken over by pathogens.
There are three types of helper T-Cells (Th1, Th2 and Th17). I'm not going to go into the details of what each of these cells do, but just remember the cytokine that they produce during a pro-inflamitory response is Gamma Interferon.
The second type of cell is called regulatory T-cells (or Tregs). The purpose of these cells are to monitor the immune system and allow Th cells (as well as B-cells) to function correctly to eliminate pathogens. But they also provide a role in shutting down an immune response when it gets out of control, such as when cells attack the body (autoimmune response).
So all T-cells are first developed in the bone marrow and then go to the thymus (this is why they are called T-cells) where they are conditioned to recognize self antigens (protein fragments of the body) so that they do not attack the self.
This is called central tolerance.
The regulatory T-cells that are developed in the thymus are often called natural regulatory T-cells (nTregs) and express certain proteins on their surface which are CD4+, CD25+ and FoxP3+. The plus sign indicated that these cells express the proteins and it is how they are identified from other cells. So, a naturally occuring regulatory t-cells that is developed in the thymus is reffered to as a CD4+CD25+FoxP3+ t cell.
These regulatory t-cells produce a cytokine known as Interleukin-10 or IL-10. This is a chemical signal that supresses the action of effector cells (helper T-cells) and shuts-down their activity.
So, it appears that some of the Th cells conditioned in the thymus to know self from non-self escape with a propensity for attacking tissues of the human body. The system is not perfect, so it is believed that the natural regulatory t-cells are better at distinguishing the self and prevent autoimmunity by shutting down these Th cells that escape.
Incidentally, there is a human disease called IPEX in which people lack the FoxP3 protein and can die very quickly of a massive autoimmune attack.
So, central tolerance is controlled by conditioning T-cells by conditioning them in the thymus.
However, there also is another mechanism that modulates the immune system which is called peripheral tolerance. This involves T-cells that are induced for normal Th cells at a localized area of inflamation. These cells are also called regulatory T-cells but are referred to as induced regulatory t cells or iTregs. Some of the cells are called Tr1 (regulatory t-cells type 1) and they produce large amounts of the suppressing cytokine IL-10. The cells express CD4+ and CD25+ and are known as CD4+CD25+ regulatory t-cells.
So there is a company trying to actively manipulate these cells as a therapy for many types of autoimmune diseases:
http://www.txcell.com/index.php?option= ... Itemid=145
So to tie this all together, it appears that people with MS have defficient numbers of Tregs (or they are not as potent):
http://www.ncbi.nlm.nih.gov/pubmed/18200504
But it appears that Vitamin D has the ability to produce Tregs and I have a lot of information on another thread that supports this:
http://www.thisisms.com/ftopic-15479-0.html
So from the link you provided, it looks like that this therapy also promotes development of regulatory T-cells:
During a 4.6-year follow-up period, parasite-infected MS patients showed a significantly lower number of exacerbations, minimal variation in disability scores, as well as fewer magnetic resonance imaging changes when compared with uninfected MS patients. Furthermore, myelin basic protein-specific responses in peripheral blood showed a significant increase in IL-10 and TGF-beta and a decrease in IL-12 and interferon-gamma-secreting cells in infected MS patients compared with noninfected patients. Myelin basic protein-specific T cells cloned from infected subjects were characterized by the absence of IL-2 and IL-4 production, but high IL-10 and/or TGF-beta secretion, showing a cytokine profile similar to the T-cell subsets Tr1 and Th3. Moreover, cloning frequency of CD4+CD25+ FoxP3+ T cells was substantially increased in infected patients compared with uninfected MS subjects. Finally, Smad7 messenger RNA was not detected in T cells from infected MS patients secreting TGF-beta.
So, I think this may also be a viable future treatment based on the results showing improved regulatory T-cell function with the treatment group.
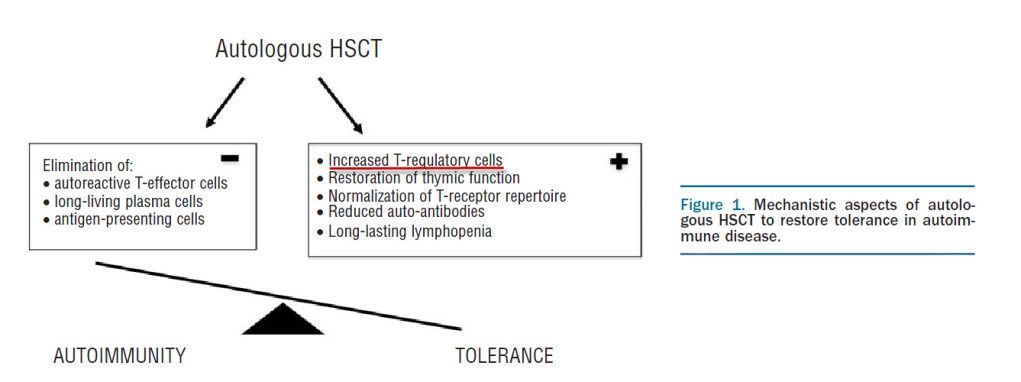
But I believe the HSCT therapy probably resets the Tregs so that they revert back to their initial efficacy. I also believe that the reason why it may not work so well in people with primary progressive disease is because there may be a proplem in the thymus which prevents development of natural T-regs. But this is just a guess and I think the scientists are on the right track to find the cause of MS.