Page 96 of 557
Posted: Wed May 19, 2010 5:41 am
by Cece
drsclafani wrote:As soon as my protocol is approved by my IRB, I am going to submit another one that will oversee the collection of the data we will collect from the squeaky one's efforts. Amazing
This is awesome...squeakycat, much applause!!!
Posted: Wed May 19, 2010 8:30 am
by Nunzio
Dear Dr. Sclafani,
yesterday I had my liberation treatment done locally.I have to report the procedure went well and I did not have any discomfort after the procedure.
Unfortunately they did not find any problem to treat.
My right IJV was narrow due to poor flow from the transverse and sigmoid sinus, so I knew there was nothing to do there.
The left IJV is large (about 1.5 cm. in diameter) with no postural change in diameter and extensive reflux. This made me think to a valve problem, but they told me, after surgery that they checked the valves with IVUS and contrast injection and found no problem. Same for azygous vein.
So my question is: How is it possible I have such an extensive reflux with no blockage? Is it possible there was a thin membrane that was open by the procedure? Could I have something similar to the Thoracic outlet syndrome? I mean some external force pushing on the vein?
Looking foreword for your answer.
Nunzio
Posted: Wed May 19, 2010 9:16 am
by Cece
drsclafani wrote:none of us want treatments that are not proven, do we?
We could put this up as a poll here...we might find quite a few people who want the unproven venoplasty treatment.

Re: history of approval process for other angioplasty proced
Posted: Wed May 19, 2010 9:29 am
by fogdweller
drsclafani wrote:fogdweller wrote:ThisIsMA wrote:My apologies if this question has already been asked.
My understanding is that balloon angioplasty is a technique that has been used for decades to expand arteries and veins in many other areas of the body.
In the past, as each new location within the body for using balloon angioplasty to treat a condition was begun, were clinical trials required? Was IRB approval required? Were doctors initially prevented from doing the procedure at a new anatomical location?
Or is this a unique process that is happening with CCSVI and MS?
I have been asking this same question, and have not gotten a good response yet. I supose the hospital administrator or whoever gives permission to do a particular procedure (Not all hospitals allow their doctors to do all procedures depending on abilities and equipment and the like). If the procedure had no known benefit, I supose the adminstrator could forbid doctors at that hospital from doing that procedure (I suspect this is what hapended at Stanford). Totally new procedures or experimantal procedures go through the IRB I think.
Angioplasty is a very safe procedure. New uses for an accepted and safe procedure should not be a big problem. Inadequate circulation in the brain is something that it seems to me should be releived if we know how.
Somehow because it has become associated with treating MS we are angsting over it.
We need to do studies to get information, but we should also offer the angioplasty to people with CCSVI if they are not participating in a study.
a doctor can treat someone with a standard technique for a new indication. HE CANNOT TREAT A GROUP without IRB.
Thank-you.
I wonder if it wouldn't be faster and easier to prove that liberation procedure relieves CCSVI as a cohort. What else might be caused by CCSVI that we could be treating?
Posted: Wed May 19, 2010 11:03 am
by drsclafani
CureOrBust wrote:drsclafani wrote:Funny, after all the years of competition, i just posted my ideas before publication....
....snip....
5.
Ah-ha! but I note you "accidentally" left number 5 blank. Like the ending of a B-grade horror movie.

did you really think I would give up all my ideas without publication?
I would actually if i thought it would make a difference
Posted: Wed May 19, 2010 11:47 am
by fogdweller
drsclafani wrote:Algis wrote:A quick Q Doctor if I may:
Am I correct to assume that the longer the stent is; the more stable it will be in the vein? Is there any constraints to that length?
Thank you for your time (and patience)
Algis
yes, that is true BUT
the longer the stent the more surface area that can go wrong, restenose etc
the larger the diameter the more stable,
the greater the lateral pressure on the vein the more stable
Do veins tend to "give out"? In other words, do the sides of the vein become even more flacid and expand away from the stent surface, so the stent can be expelled as a foreign body I would think stent migration might be very common.
Posted: Wed May 19, 2010 2:48 pm
by pegmegrund
Hi Dr. Sclafani,
Thank you for this thread. I'm glad you're here answering our questions.
My question is: I have premature ventricular contractions (PVCs) and PACs and had them checked out about 5 years ago. I wore a holter monitor for 24 hours. My heart checks out fine. My blood pressure is normal. I was told to stop caffeine... (didn't happen) and I also notice that these 'flutters' happen more when I'm stressed.
Does the existence of this type of irregular heartbeat in an otherwise health heart affect my ability to have catheter venography to treat CCSVI?
Thanks!
Pam
Posted: Wed May 19, 2010 3:10 pm
by Cece
fogdweller wrote:Do veins tend to "give out"? In other words, do the sides of the vein become even more flacid and expand away from the stent surface, so the stent can be expelled as a foreign body I would think stent migration might be very common.
Do you mean do they give out over a longer period of time? It's only a matter of weeks until the stent is incorporated into the vein and can't be budged. They're also using stents that are slightly larger than the vein so that they wedge in better, if I understand correctly. If stent migration were common, we'd have heard reports of it out of Poland by now?
Posted: Wed May 19, 2010 6:10 pm
by astro
drsclafani wrote:Nice images.
First, the narrowings are not high grade compared to many others i have seen. What is your EDSS?
My EDSS score is 3.5. Given the increased symptoms in my legs since my IJV treatment, however, it has unfortunately been creeping toward 4.0 in the last six weeks. Coincidence? The engineer in me says no, but I digress.
drsclafani wrote:I see a clear cut stuck valve on the left side. They are pesky sometimes, need cutting balloons and possibly will ultimately need stents. The reflux in the subclavian is physiological, depending upon the cardiac output, and the volume of contrast injected. The subclavian veins should not have valves there so reflux is not surprising and is seen often during these studies.
Zamboni says he is often seeing an abnormal asygous
Thank you for your insight, Dr. Sclafani. I wonder about the implications of the stuck valve that you noted. What is the purpose of this valve when it is working properly? Are there specific conditions (sitting vs supine, resting vs physical exertion) under which the stuck valve is more problematic?
As you also noted, my IJV narrowing is not as severe as others, which is why I attribute at least some of my disability to either the valve you mention or something in my azygos. Here are two of my azygos images.
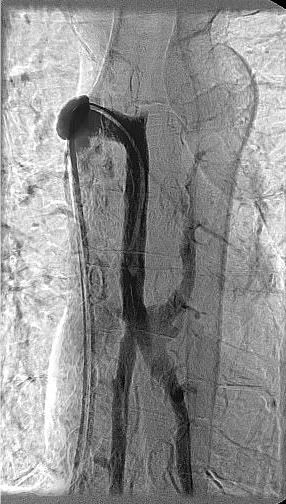

I understand from your experience that these images must be from the correct angle to identify blockage. Do these appear to be taken from the correct angles? Am I “lucky” enough to have any azygos abnormalities reveal themselves to your trained eye?
Posted: Wed May 19, 2010 6:36 pm
by 1eye
Still....
I have read about all kinds of "back-alley" treatments (i.e. sans irb). Does anyone know of a treatment center in the US that has not been shut down yet? PM me if you do.
willing to travel, even on an empty stomach...
Posted: Wed May 19, 2010 6:58 pm
by newlywed4ever
drsclafani wrote:Cece wrote:newlywed4ever wrote:MORE Importantly! I agree with you about a study using fake venoplasty by not inflating; I cringed when I read that post.
Yeah, I wouldn't want to be in that study, and I was the one who thought it was noteworthy enough to bring up here.
I'm in favor of randomized trials if that's what it takes to get this accepted but I'd rather it not be necessary. And I don't know that it is. As far as I can google, angioplasty has never been subjected to randomized trials yet it has been in use for thirty years.
It is a different world there now. Many of us did investigation in an informal way in the past but hospitals and medical groups and societies now insist on it. Journal do not publish material without statements that the studies were done under IRB oversite.
Thanksfully, there WILL be people who will want to be in randomized double blinded trials. Either because they like it, or they feel an ethical responsibility to participate in new treatment evaluations or because (fill in the blank)
There have been many trials of angioplasty, but not as rigorous as is expected in the current era. On the other hand a recoent publication compared unconvered stents versus covered stents for restenosis of dialysis grafts. The data was informative, trustworthy and thus advanced the treatment in a secure way.
The new health care reforms require that many ideas be tested to prove efficacies and advantages over other therapies. none of us want treatments that are not proven, do we?
Dr S - again, you enlightened/educated me. It all makes sense until your last statement. Yeah, we want it. Whether or not it's recognized as "proven" or not. We haven't seen this much proof since 95% of us (my math/not proven) have been diagnosed. And, yeah, we're a bit desparate.
Posted: Wed May 19, 2010 8:39 pm
by 1eye
I don't like that word: desperate. Usually used to put somebody down. Comes from the verb, to despair. In spite of all the lies, spin, hype, and forced travel, I don't think I've seen much despair. The community at large is busy failing us big-time. Though I think research is all fine and dandy, there are many people suffering at this moment. I have lots of symptoms, yes, but I am stable, progression is (currently) slow, and pain is manageable. But there are thousands and thousands, all over the world. There is a lot of suffering. Do you, Dr. Sclafani, think interventional radiologists and vascular surgeons have a moral imperative to provide this treatment? I do. Here in Canada, we had one brave doctor who went to jail over providing abortion care. Of course I don't want to argue the morality of abortion, but can't somebody see that these people are needlessly suffering? Because some busybody loud-mouthed hysterics accuse people who are doing good medicine of being wrong and unsafe, and threaten their licenses? Can one go to jail for practising good medical care? Do I live in the nineteenth century? This has got to stop, and some sanity must return to medicine.
A famous neurologist, speaking before a Canadian parliamentary committee, said:
"If all patients are given the therapy, no one will go in a trial."
This statement is insane. Obviously insane.
What can we do beside seek treatment in another country? Our own countries have let us down. I think your, and many other research projects are necessary. But many people cannot wait. Now MS Societies have embraced CCSVI, but still no-one is advocating for the most needy victims. Why? Do they not count? Have they somehow become less human?
Maybe I should despair. I've heard desperate people do desperate things. I hope. I try to hope.
Posted: Wed May 19, 2010 9:08 pm
by Algis
a doctor can treat someone with a standard technique for a new indication. HE CANNOT TREAT A GROUP without IRB.
Why not to treat 50 (500) 'individuals' then

Not trying to be a smart ass but isn't a group merely a suite of individuals? That's just picky'ing around (just invented that one to suite my needs; without approval
).
Re.Stents: Are the stents a 'spring' or a 'mesh'. Spring would keep pushing the walls after deployment; a mesh would keep its deployed diameter after removal of the tool.
Just trying to educate myself, I've never seen the manipulation of stents.
Thank you Doctor.
Posted: Wed May 19, 2010 9:38 pm
by hope410
Algis wrote:[Why not to treat 50 (500) 'individuals' then
Not trying to be a smart ass but isn't a group merely a suite of individuals? That's just picky'ing around (just invented that one to suite my needs; without approval
).
I'm very surprised at this distinction between one versus many too. If you had one patient who benefited from an off-label use of something or new use for established procedure, wouldn't you have an obligation to treat others/everyone the same way?
And did casting a broken left leg to set it while it healed require a different IRB process than a broken right leg?
Or is my analogy not the same as this situation, i.e., a broken left leg is the same as a broken right leg, but a blocked liver vein is not the same as a blocked azygous vein? So ballooning different veins is very unique and therefore ballooning different veins needs separate IRB protocols and investigations? Is each different vein going to require its own IRB oversight, or at some point, is a vein just a vein just a vein?
I'm really confused by what the problem is when veins ARE ballooned already and have been, as you said, for decades.
Posted: Thu May 20, 2010 3:11 am
by Algis
What else might be caused by CCSVI that we could be treating?
Just go to the emergency room; sit and shout "my jugulars hurts, help!!"...?