Page 99 of 557
Posted: Sat May 22, 2010 8:46 pm
by drsclafani
Nunzio wrote:Dear Dr. Sclafani,
yesterday I had my liberation treatment done locally.I have to report the procedure went well and I did not have any discomfort after the procedure.
Unfortunately they did not find any problem to treat.
My right IJV was narrow due to poor flow from the transverse and sigmoid sinus, so I knew there was nothing to do there.
The left IJV is large (about 1.5 cm. in diameter) with no postural change in diameter and extensive reflux. This made me think to a valve problem, but they told me, after surgery that they checked the valves with IVUS and contrast injection and found no problem. Same for azygous vein.
So my question is: How is it possible I have such an extensive reflux with no blockage? Is it possible there was a thin membrane that was open by the procedure? Could I have something similar to the Thoracic outlet syndrome? I mean some external force pushing on the vein?
Looking foreword for your answer.
Nunzio
Sorry that your liberation did not make any changes to your condition. What is your MS classification.
i did have one case early in my experience where venography looked normal on several views. one one view there was the thinnest of horizontal webs. It seemed that it was possible for a web to be pushed up by the catheter and be "invisible". I was very lucky indeed to see this.
Posted: Sat May 22, 2010 8:49 pm
by drsclafani
Cece wrote:drsclafani wrote:none of us want treatments that are not proven, do we?
We could put this up as a poll here...we might find quite a few people who want the unproven venoplasty treatment.

cece
i fully understand your position on this. Unfortunately doing unproven treatments that are NOT the standard of care are fraught will opportunities to do harm, manipulate patients, lead to a negative backlash, etc. Thus such situations are usually handled by oversight committies such as an IRB or by a new procedure committee,
otherwise medicine would turn into a hair salon
Posted: Sat May 22, 2010 8:58 pm
by drsclafani
I wonder if it wouldn't be faster and easier to prove that liberation procedure relieves CCSVI as a cohort. What else might be caused by CCSVI that we could be treating?
i do not understand this question.
are you suggesting that we look at patients with CCSVI as the cohort, rather than MS?
I think that it is too late for that. Also, while there are non MSers who can have CCSVI, such patients are uncommon. I do not think that the authorities overseeing health care are going to see that technique as anything other than a subterfuge.
They certainly did not buy my argument of just that as a reason to go forward without IRB
Posted: Sat May 22, 2010 9:07 pm
by drsclafani
fogdweller wrote:drsclafani wrote:Algis wrote:A quick Q Doctor if I may:
Am I correct to assume that the longer the stent is; the more stable it will be in the vein? Is there any constraints to that length?
Thank you for your time (and patience)
Algis
yes, that is true BUT
the longer the stent the more surface area that can go wrong, restenose etc
the larger the diameter the more stable,
the greater the lateral pressure on the vein the more stable
Do veins tend to "give out"? In other words, do the sides of the vein become even more flacid and expand away from the stent surface, so the stent can be expelled as a foreign body I would think stent migration might be very common.
Yes, that is a possibility.
I can think of several scenarios by which a stent could migrate
1. while removing the balloon catheter, the stent catches upon the balloon and is dragged downward to a larger diameter part of the vein from which it could migrate
2. The stent size was miscalculated and was too small to begin with OR the oversizing of the stent was not adequate
3. The stent size was correct to begin with but the vein dilated afterward. This could occur if the outflow obstruction was corrected and as more flow went through the vein, it dilated as expected and thus the stent was no longer held in place by the wall of the vein
4.
Posted: Sat May 22, 2010 9:09 pm
by Trish317
drsclafani wrote:Cece wrote:drsclafani wrote:none of us want treatments that are not proven, do we?
We could put this up as a poll here...we might find quite a few people who want the unproven venoplasty treatment.
cece
i fully understand your position on this. Unfortunately doing unproven treatments that are NOT the standard of care are fraught will opportunities to do harm, manipulate patients, lead to a negative backlash, etc. Thus such situations are usually handled by oversight committies such as an IRB or by a new procedure committee,
otherwise medicine would turn into a hair salon
That really made me laugh, Dr. S. I'm a natural redhead who, in my 30's, had to start looking for ways to "fix" what was happening to my hair. God forbid that medicine would turn into a hair salon.
Thank you for everything you're doing, and thank you for everything you write here, with honesty and integrity, to support, teach, comfort, and assuage fears.
Posted: Sat May 22, 2010 9:12 pm
by Cece
drsclafani wrote:Cece wrote:drsclafani wrote:none of us want treatments that are not proven, do we?
We could put this up as a poll here...we might find quite a few people who want the unproven venoplasty treatment.
cece
i fully understand your position on this. Unfortunately doing unproven treatments that are NOT the standard of care are fraught will opportunities to do harm, manipulate patients, lead to a negative backlash, etc. Thus such situations are usually handled by oversight committies such as an IRB or by a new procedure committee,
otherwise medicine would turn into a hair salon
I know, I was just teasing.
I think it is crucial to prove it so that it can be gotten out to the masses as soon as reasonably possible. (MaSses?) Otherwise it would stay as it is, with a trickle of motivated patients willing to go for it but most people unaware.
as for what cut I want at the hair salon, I would like long & flowing & untangled (veins)
Posted: Sat May 22, 2010 9:12 pm
by drsclafani
pegmegrund wrote:Hi Dr. Sclafani,
Thank you for this thread. I'm glad you're here answering our questions.
My question is: I have premature ventricular contractions (PVCs) and PACs and had them checked out about 5 years ago. I wore a holter monitor for 24 hours. My heart checks out fine. My blood pressure is normal. I was told to stop caffeine... (didn't happen) and I also notice that these 'flutters' happen more when I'm stressed.
Does the existence of this type of irregular heartbeat in an otherwise health heart affect my ability to have catheter venography to treat CCSVI?
Thanks!
Pam
AS the catheter goes through the heart, it is possible that the guidewire or the catheter can "tickle" the right atrium and this can result in some irregular heart beats that usually stop immediately after the wire and catheter exit the heart on the way to the jugular and azygous veins.
Given that you are prone to irregular heart beats as PVCs or PACs, i would think that the procedure might be more risky. However i would think that having a cardiologist on standby to address such situations would be prudent. I would not consider it an absolute contraindication to the procedure
Posted: Sat May 22, 2010 9:54 pm
by librajen
Thank you, Dr Scalfani, for caring so much to answer our questions. I have spent a lonely Saturday night reading all 99 pagers of this forum, and have learned so much. (((hugs))) to you...blushing...
I have been tested in Buffalo, NY, and my right jugular vein was found to be narrowed (moderate to severe stenosis), and I have booked a date for Liberation in San Jose, Costa Rica.
My question is: Do you think that continuing an interferon drug (Avonex, in my case) is wise after Liberation? It's making my hair fallout LOL
Posted: Sat May 22, 2010 9:58 pm
by drsclafani
astro wrote:
Thank you for your insight, Dr. Sclafani. I wonder about the implications of the stuck valve that you noted. What is the purpose of this valve when it is working properly? Are there specific conditions (sitting vs supine, resting vs physical exertion) under which the stuck valve is more problematic?
The purpose of vein valves is to prevent significant reversed flow.
the stuck valve prevents drainage while preventing reflux. The stuck valve is more problematic when your brain outflow is directed to the veins that are abnormal. For example, in the supine position blood normally drains through the jugular vein. Thus stiff or stuck valves in the IJV are problematic why lying down.
As you also noted, my IJV narrowing is not as severe as others, which is why I attribute at least some of my disability to either the valve you mention or something in my azygos. Here are two of my azygos images.
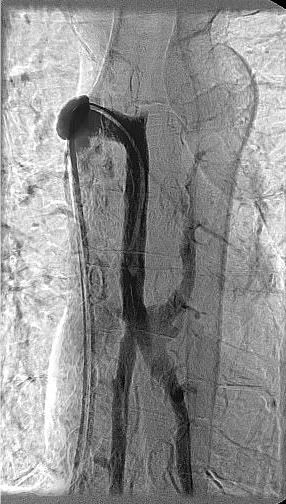

I understand from your experience that these images must be from the correct angle to identify blockage. Do these appear to be taken from the correct angles? Am I “lucky” enough to have any azygos abnormalities reveal themselves to your trained eye?
ok, let me show you an image of an azygous well visualized.

[/img]
can you see the difference? There are three sets of valves in the azygous arch.
Posted: Sat May 22, 2010 10:18 pm
by drsclafani
Algis wrote:a doctor can treat someone with a standard technique for a new indication. HE CANNOT TREAT A GROUP without IRB.
Why not to treat 50 (500) 'individuals' then

Not trying to be a smart ass but isn't a group merely a suite of individuals? That's just picky'ing around (just invented that one to suite my needs; without approval

).
doctors dont treat groups. maybe shrinks do....ie group therapy, but most of us treat a patient and each patient is assessed and treated individually. Once you get into group dynamics, the stadards of the world is you are doing an experiment and doing experiements on vulnerable groups is fraught with danger
Re.Stents: Are the stents a 'spring' or a 'mesh'. Spring would keep pushing the walls after deployment; a mesh would keep its deployed diameter after removal of the tool.
stents are metallic tubular constructs that when deployed exert radial pressure against the vessel wall
Posted: Sat May 22, 2010 10:25 pm
by drsclafani
hope410 wrote:Algis wrote:[Why not to treat 50 (500) 'individuals' then
Not trying to be a smart ass but isn't a group merely a suite of individuals? That's just picky'ing around (just invented that one to suite my needs; without approval
).
I'm very surprised at this distinction between one versus many too. If you had one patient who benefited from an off-label use of something or new use for established procedure, wouldn't you have an obligation to treat others/everyone the same way?
no, because it is unproven and not the standard of care. Using it on everyone would imply that it is the standard of care
And did casting a broken left leg to set it while it healed require a different IRB process than a broken right leg?
Or is my analogy not the same as this situation, i.e., a broken left leg is the same as a broken right leg, but a blocked liver vein is not the same as a blocked azygous vein? So ballooning different veins is very unique and therefore ballooning different veins needs separate IRB protocols and investigations? Is each different vein going to require its own IRB oversight, or at some point, is a vein just a vein just a vein?
I'm really confused by what the problem is when veins ARE ballooned already and have been, as you said, for decades.
no one needs an IRB to treat a vein problem. What causes the controversy is that you have a new treatment in a group of patients (MS) for which there is no standard of care
Posted: Sat May 22, 2010 10:27 pm
by drsclafani
thisisalex wrote:Hello Dr. Sclafani,
im a big fan of your presence here, and would like to ask a question.
A neurosonographer has jus published a critical approach to Zamboni's Doppler methodology.
He thinks that 3 out of the 5 Zamboni criterias are completely nonsense, and are not for diagnosing an occlustion in a vein.
He also states that none of the Ultrasound pictures published by Zamboni convinced him that a vein occlusion has been observed.
He gives detailed description about his doubts here:
http://www.thisisms.com/ftopic-11804-0- ... rasc-.html
May i ask your professional opinion about these statements? It would be very important to reply to his opinion, because in hungary we have just started to organize a CCSVI trial... and would like to finish it
thank you very much!
alex
This one requires some thought and discussions before i post
Re: Siskin
Posted: Sat May 22, 2010 10:44 pm
by drsclafani
thirdday wrote:FlashHack wrote:Very interesting. Dr. Siskin mentioned to me about finding people where CCSVI was detected by doppler US but not seen on the venogram. He spoke of it as a indication of how unreliable the doppler was, but this would seem to indicate that the venogram was the inaccurate one. Could this be what he encountered?
My question would be, was something missed in the venogram? Was enough dye used? Did the dye go into the correct places? Or are both the ultrasound & venogram results dependant on the doctors interpretation and experience?
everything is dependent upon experience and interpretation. That is why medicine is called an art and a science.
One of the ways to hide some of the problems is to inject TOO much dye. It becomes so opaque that the valves and septa cannot be seen.
however i still feel confident that venography will show many things that are not recognizable on ultrasound examination.
Posted: Sat May 22, 2010 10:46 pm
by drsclafani
LR1234 wrote:Hi Dr Sclafani,
Would you mid answering a couple of questions
1.If a vein is over stretched during an angioplasty so that it is too wide to place a stent Can this be as detrimental as a blocked or stenosed vein? (As in the case of Rici) especially if reflux still exists.
that is a possibility. I still wonder whether ricci has right heart failure that would make his reflux so great.
2. It seems that for many MSers blood flow is a problem not just inverted valves/stenosis/blocked veins.
Are their currently any drugs on the market that could increase the flow through the veins?
I know we have drugs that can raise and lower BP (fludrocortisone/Liprinisol) etc which change the flow through the arteries but I don't think effects the veins do they?
Also Thyroxine raises the heart rate would this help with venous flow?
Could adding some sort of fluid via IV to MS patients veins reguarly help to clean the blood and keep it moving??? (maybe some sort of saline solution or mineral solution)
Thanking you in advance
L
i do not think this would be effective......now i sound like a neurologist!
Posted: Sat May 22, 2010 10:48 pm
by drsclafani
miranda wrote:Dear Dr. Sclafani
My son is on your waiting list but unfortunately we did not anticipate such a delay. He fractured his right clavicle about 10 years ago. The orthopaedic
placed a screw which he later removed. He was diagnosed with MS
Sept 2009. I have mailed all his medical reports to Holly. Since he is
in a state of panic as soon as he found out about the delay, he had a
CCSCI DOPPLER EXAM by an inexperienced IR. According to his
findings there was cerebral blod flow disturbances He suggested
an MRV.
Is there a gold standard diagnosis for CTOS? Should he be tested /treated ?
sorry but i am not familiar with CTOS. what does this mean?