Page 276 of 557
Posted: Sun Dec 12, 2010 10:44 am
by Nunzio
Hi Dr. Sclafani,
I had my CCSVI treatment done a week ago and my case was identical to the one you presented with an hypoplastic vein. It was elected to leave that vein alone and to dilate the constricted valve at the confluens with the brachiocephalic vein with I would guess that it was 20 to 30% narrowed.
I had incredible improvements the first day including the disappearance of my enlarged left periorbital vein, but then my improvement disappeared and I think now I am back to pretreatment status.
drsclafani wrote:
unless your distend the annular constriction beyond its elasticity, you will not break the band and elastic recoil is the rule. Some of this tissue is really elastic and really high pressure is necessary. Yesterday, it required 25 atmospheres to overcome the tissue band causing the obstruction
The balloon however does not have to be larger than your vein. Once the annular constriction is broken, the constricted vein seems to distend in the area of the constriction. So I might try an 18 or 20 mm balloon on your vein.
I think the reason is that since the dilation was only 20% that was not enough to break the annulus band as a 50% narrowing would have allowed and even my periorbital vein are back.
I do not know yet what size balloon and what pressure was used and I will be able to give you more info once I get my DVD of the procedure.
At this point I am thinking to repeat the doppler to see if there is any change in my left jugular vein.
I am grateful to you for sharing your knowledge with us.
Posted: Sun Dec 12, 2010 11:38 am
by NZer1
Finding patients with similar problems and approaching them differently, checking outcomes.
If a collateral grows or enlarge (because it already exists) and there is virtually no BP in the vein, why is there problems getting veins to stay open? For a vein to stay open it must also overcome the flesh, muscle, bone around it?
Is there a yet to be understood process that creates collaterals, for them to be able to grow and 'expand' when there is a no pressure flow?
Or is there a process that allows veins to grow to cater for flow when there is no pressure inside? What makes veins stay open when there is no pressure to hold then to a size? Or is there a problem time where blood cannot flow, which creates pressure and expands the vessel, eventually finding flow paths over time and then pressure decreases? There has to be a stage thing going on here as we grow I guess? What happens when we exercise and more blood volume passes? Is this a time of enlarging of the veins and the growth to allow flow happens?
As we grow is there a problem occurring that the veins stop growing? Hence the age onset? Or the female / male imbalance and puberty?
Posted: Sun Dec 12, 2010 12:28 pm
by Cece
drsclafani wrote:depends if you are from canada or canarsie.
That was clever.

progressive dilatation is performed to mature arteriovenous fistulas for dialysis. dilatation of 2-4 millimeters is done at two week intervals.
The patient in question is closer to Canarsie than to Canada, should we expect a two-week update?
Much appreciation to your AAC colleagues for their knowledge of this method.
Posted: Sun Dec 12, 2010 12:50 pm
by mo_en
Supposing the quide wire can not find its way through a hypoplastic and (obviously) occluded jugular vein, is there any benefit in trying with a thinner wire like 0.018"? After all the smaller sized initial balloon would fit just right in the line of successive and progressive dilatations.
Posted: Sun Dec 12, 2010 5:52 pm
by LauraV
Dr. Sclafani,
A friend sent me a post that she read on another site about a doctor in California (?) who has a different approach to unblocking veins. He tears the valves. He claims to have 100% success. None of his patients have experienced re-stenosis.
http://ccsvi-ms.ning.com/profiles/blogs ... california
Do you know this doctor? What do you think of this technique?
Laura
Posted: Sun Dec 12, 2010 7:04 pm
by Cece
Laura, this sounds like what Dr. Sinan does with the valvulotomy balloon, I ask Dr. Sclafani about this every few months.
drsclafani on Aug 11 wrote:Cece wrote:* Did Dr. Sinan talk any more about valvulotomy? Does it seem like valvulotomy is acceptably safe?
no, the talk was about "cutting balloons" more than valvulotomy balloons. I do not have any experience with that balloon.
drsclafani on May 28 wrote:Dr Sinan has told me he is using a valvulotomy device to cut the stuck or stiff valves. I am looking into that recommendation but havent used it since I AM STILL ON THE FREAKIN SIDELINE.
Although on second thought, tearing might be different than cutting.
100% no restenosis seems unlikely, doesn't it?
Here we go:
drsclafani wrote:Angioplasty attempts to tear the valve's attachment to the wall or split apart any fusion of the leaflets, or stretch wall
adjacent to it. So it is not one question, one problem, or one solution. I do see improved flow, but we will have to
wait to understand the natural history of the treatments.
I don't think what Dr. Arata is doing is any different than what any of the docs are doing?
Posted: Sun Dec 12, 2010 11:27 pm
by drsclafani
[quote="drsclafani"]
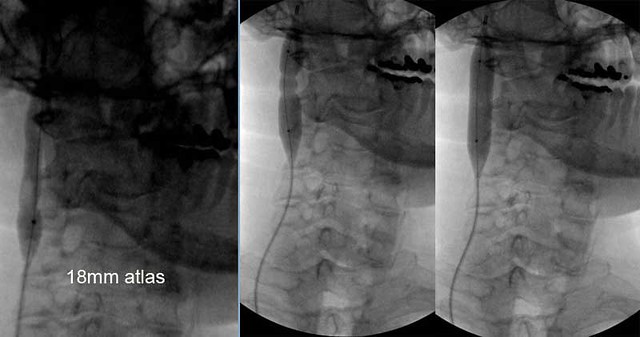
in this case we dilated the vein to 12 millimeters. We reached high pressures around 20 Atmospheres. no balloon "waisting" was seen except at the truncular areas. While there was waisting, it did not go away even with very high pressure. Failing to break that stenosis, will result in early elastic recoil.

followup venography after the angioplasty (on the right) did not show much change except that less collateral veins were seen compared to the original venogram on the left.

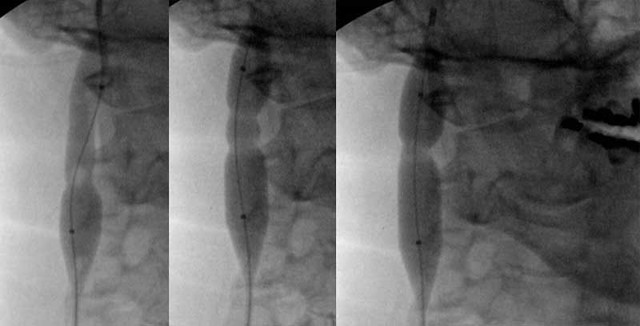
So I proceeded to dilate another six millimeters. Despite no evidence of stenoses an 12 mm dilation, multiple areas of annular restrictions were identified by inflating the angioplasty balloon. These were treated by 18 mm balloon angioplasty under high pressures
Here is a closeup of upper area of hypoplasia
this is the image of the lower area
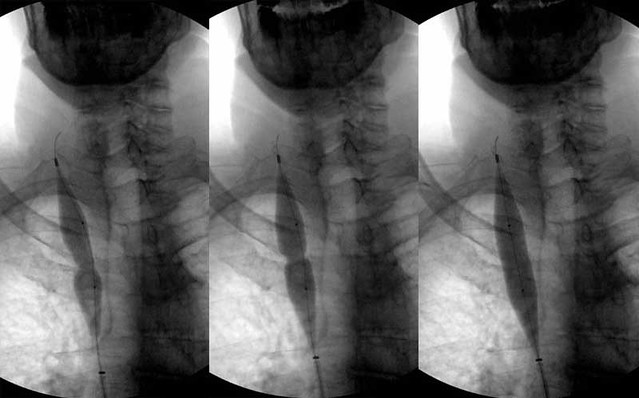
A venogram is always repeated after angioplasty to see the amount of dilation, to look for leakage and to look for clots

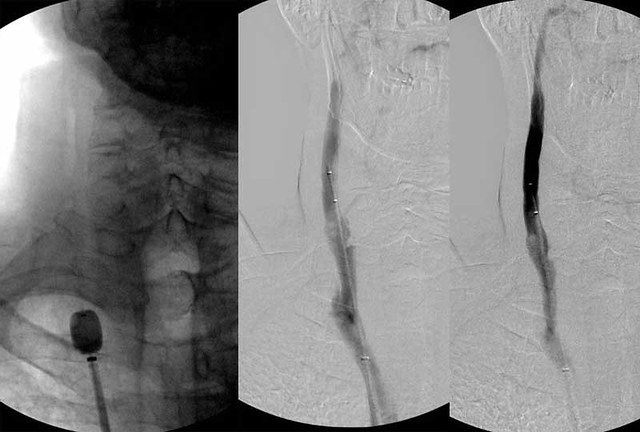
looks pretty ugly to me, irregularities, small filling defects in the contrast, all suggested that clot was forming. The ballooning was repeated with low pressure, to sort of iron out the vein. the image on the right shows that the upper part looks pretty good but the lower part still looks like crap.
So Finally a thrombectomy catheter was placed in there and further clot was stripped out. The final image looks better. you can still see the hypoplasia in the upper part of the vein. I just do not know how to deal with that yet..
Posted: Sun Dec 12, 2010 11:31 pm
by drsclafani
Nunzio wrote:Hi Dr. Sclafani,
I was reading a PDF presentation from Dr. Al-Omari from Jordan and I was intrigued by his statement on facial signs of CCSVI because I have exactly the same symptoms on my left lower lid: Please look from page 54 to page 57 of the link below.
Q:Is there any facial sings of CCSVI
A:YES:
Subcutaneous
Periorbital and frontal
Veins:
Dilated Periorbital vein
in CCSVI patient
Not uncommon clinical
finding
Respond well to
liberation procedure
http://www.essentialhealthclinic.com/we ... -omari.pdf
I looked a bit more into it and I found the anatomical reason for it: those vein are branching off the anterior facial vein which originate from the Interior jugular vein as you can see from the picture below

So my question is if you noticed this too in some of your patients and if you noticed the disappearance of those vessels after a successful procedure.
Thanks a lot.
nunzio
i have noticed dilated veins not just that one. i havent really focused on clinical signs as i am going to do venography and ultrasound. They are better than physical exam.
but thanks
i will start to look more carefully
Posted: Sun Dec 12, 2010 11:36 pm
by drsclafani
Nunzio wrote:Hi Dr. Sclafani,
I had my CCSVI treatment done a week ago and my case was identical to the one you presented with an hypoplastic vein. It was elected to leave that vein alone and to dilate the constricted valve at the confluens with the brachiocephalic vein with I would guess that it was 20 to 30% narrowed.
I had incredible improvements the first day including the disappearance of my enlarged left periorbital vein, but then my improvement disappeared and I think now I am back to pretreatment status.
drsclafani wrote:
unless your distend the annular constriction beyond its elasticity, you will not break the band and elastic recoil is the rule. Some of this tissue is really elastic and really high pressure is necessary. Yesterday, it required 25 atmospheres to overcome the tissue band causing the obstruction
The balloon however does not have to be larger than your vein. Once the annular constriction is broken, the constricted vein seems to distend in the area of the constriction. So I might try an 18 or 20 mm balloon on your vein.
I think the reason is that since the dilation was only 20% that was not enough to break the annulus band as a 50% narrowing would have allowed and even my periorbital vein are back.
I do not know yet what size balloon and what pressure was used and I will be able to give you more info once I get my DVD of the procedure.
At this point I am thinking to repeat the doppler to see if there is any change in my left jugular vein.
I am grateful to you for sharing your knowledge with us.
i am going for broke. i am using very high pressure balloons. I have shown you that you can eliminate many of the waists on the balloons if you use too small a diameter. One can actually think you are doing a good job, but when you put in the larger balloons, it is clear that the stenosis is still present, just stretched a bit. Often when the stenosis is really stretched, one hears a audible pop, the patient's stretch pain drops dramatically immediately and the pressure in the balloon drops to a lower level.
i am very curious to know what size balloon, what pressure was used, what type of balloon was used,
Posted: Sun Dec 12, 2010 11:43 pm
by drsclafani
mo_en wrote:Supposing the quide wire can not find its way through a hypoplastic and (obviously) occluded jugular vein, is there any benefit in trying with a thinner wire like 0.018"? After all the smaller sized initial balloon would fit just right in the line of successive and progressive dilatations.
funny that you should ask that. I had such a case yesterday. I could not cannulate the hypoplastic vein from the leg.....i had not choice but to stick the neck, and put a guidewire down . it naturally ran down through the stenosis into the chest. lucky for me as i was able to then get the angioplasty balloon up into the hypoplastic vein. these veins are not thrombosed. They are just really narrow or collapsed, so i have not encourtered an inability to run the wire up the channel.
Posted: Sun Dec 12, 2010 11:45 pm
by drsclafani
Cece wrote:drsclafani wrote:depends if you are from canada or canarsie.
That was clever.
progressive dilatation is performed to mature arteriovenous fistulas for dialysis. dilatation of 2-4 millimeters is done at two week intervals.
The patient in question is closer to Canarsie than to Canada, should we expect a two-week update?
Much appreciation to your AAC colleagues for their knowledge of this method.
i will surely let you all know if this restenoses.
i will follow with ultrasound at 1,3,6,9,12,18,24,36 months
lets hope for the best
Posted: Sun Dec 12, 2010 11:54 pm
by drsclafani
LauraV wrote:Dr. Sclafani,
A friend sent me a post that she read on another site about a doctor in California (?) who has a different approach to unblocking veins. He tears the valves. He claims to have 100% success. None of his patients have experienced re-stenosis.
http://ccsvi-ms.ning.com/profiles/blogs ... california
Do you know this doctor? What do you think of this technique?
Laura
Laura, this is what I am doing as well. the doctor that the person is writing about is treating the annular stenosis at the valve area. From IVUS, it appears that the valve does not completely open. I think we are tearing the annulus of the valve and this results in the valve falling away from the wall of the vein. It looks pretty interesting on IVUS. I will show one soon.
high pressure large balloon therapy was described at my symposium in july by dr tariq sinan (kuwait and Egypt). He is also having good results.
However not all patients respond to treatment like the patient who wrote that blog. great news for her.
Posted: Mon Dec 13, 2010 12:28 am
by CCSVIhusband
drsclafani wrote:LauraV wrote:Dr. Sclafani,
A friend sent me a post that she read on another site about a doctor in California (?) who has a different approach to unblocking veins. He tears the valves. He claims to have 100% success. None of his patients have experienced re-stenosis.
http://ccsvi-ms.ning.com/profiles/blogs ... california
Do you know this doctor? What do you think of this technique?
Laura
Laura, this is what I am doing as well. the doctor that the person is writing about is treating the annular stenosis at the valve area. From IVUS, it appears that the valve does not completely open. I think we are tearing the annulus of the valve and this results in the valve falling away from the wall of the vein. It looks pretty interesting on IVUS. I will show one soon.
high pressure large balloon therapy was described at my symposium in july by dr tariq sinan (kuwait and Egypt). He is also having good results.
However not all patients respond to treatment like the patient who wrote that blog. great news for her.
So, Dr., it's valves? Valves are the main CCSVI problem?
In the azygous I believe there are 3 valves (often malformed)?
and in the jugulars at the bottom?
What about webs?
Also ... it's 327 AM and you're posting away ... when do you sleep???
one more ... can you speak briefly to elastic recoil? The process, just anything generally ... educate us a bit please!
Posted: Mon Dec 13, 2010 1:25 am
by hope410
Dr. Sclafani - so are you using 18mm balloons routinely now? On ALL veins (incl. azygous)? Regardless of 'normal' size of healthy part of vein and since vein size is so variable? If so, doesn't this increase vein damage/risk of rupture for smaller veins?
Do we have data on reduction of re-stenosis due to usage of larger balloons, or just Dr. Sinan's observations? I think some IR's in California are also using larger balloons too. Is it riskier?
Thanks!
Posted: Mon Dec 13, 2010 8:24 am
by Cece
CCSVIhusband wrote:So, Dr., it's valves? Valves are the main CCSVI problem?
I was originally under the impression (from the MRV images and all the talk of stenosis and narrowing) that the valves were a side issue but I was strongly corrected on that along the way!
drsclafani on May 23rd wrote:cece
some of the malformations are of the valves themselves. abnormal location, abnormal leaflets, fused leaflets, etc. there are other malformations such as thickend wall and narrowed or atresia (inadequate development) but i think that this is mostly a valve problem
Also ... it's 327 AM and you're posting away ... when do you sleep???
I think he's discovered my stash of Provigil

although from the lstgert nslloongd ptovrftu the other day, he might be sleep posting...
one more ... can you speak briefly to elastic recoil? The process, just anything generally ... educate us a bit please!
drsclafani on Mar 13th wrote:yes, thrombosis can occur, especially without anticoagulation for protection in the short term. i think however, that elastic recoil is more likely. elastic recoili is the same as stretching a rubber band and then it recoils and forms its own size and shape.
drsclafani on March 23rd wrote:There are many causes of restenosis, including elastic recoil, intimal hyperplasia, neointima, thrombus,
Elastic recoil is likely happening in patients with ccsvi . Also the hypertrophied valves may get pushed against the wall, but then slowly or quickly retain their original shape and cause obstructions.
...
in CCSVI we are dealing with abnormal tissue development so restenosis can occur because of elastic recoil of that tissue. also restenosis can result when the valve that is pushed against the wall of the vein, begins to return to its original shape and orientation.
drsclafani on oct 13th wrote:the normal vein is very distensible, but the abnormal vein is resistant to stretch. The valvular stenoses are also problematic for the same reason.