Page 277 of 557
Posted: Mon Dec 13, 2010 9:03 am
by Cece
hope410 wrote:Dr. Sclafani - so are you using 18mm balloons routinely now? On ALL veins (incl. azygous)? Regardless of 'normal' size of healthy part of vein and since vein size is so variable? If so, doesn't this increase vein damage/risk of rupture for smaller veins?
Do we have data on reduction of re-stenosis due to usage of larger balloons, or just Dr. Sinan's observations? I think some IR's in California are also using larger balloons too. Is it riskier?
Thanks!
if this helps, here he talked about the likely range of balloon diameters depending upon the size of the vein:
http://www.thisisms.com/ftopicp-143961.html#143961
risk of rupture, even at 10 mm, and what to do in event of rupture:
http://www.thisisms.com/ftopicp-143493.html#143493
none has occurred yet:
http://www.thisisms.com/ftopicp-146173.html#146173
"age of discovery" (studies needed, lack of data):
http://www.thisisms.com/ftopicp-121337.html#121337
Posted: Mon Dec 13, 2010 9:06 am
by msjen
I hope I am giving you all of the information you need. I had the procedure done almost 6 months ago and they told me there was still 20% residual stenosis. Is this normal? I have since re-stenosed, but I don't recall hearing about this previously.
Posted: Mon Dec 13, 2010 9:29 am
by drsclafani
msjen wrote:I hope I am giving you all of the information you need. I had the procedure done almost 6 months ago and they told me there was still 20% residual stenosis. Is this normal? I have since re-stenosed, but I don't recall hearing about this previously.
when you finish the procedure and there is a 20% residual stenosis, it strongly suggests that the elasticity of the annulus (if you are speaking about an annular stenosis) has not been overcome. In otherwords, they have stretched the rubber band, but not torn it. it was only a matter of time

Posted: Mon Dec 13, 2010 9:37 am
by drsclafani
hope410 wrote:Dr. Sclafani - so are you using 18mm balloons routinely now? On ALL veins (incl. azygous)? Regardless of 'normal' size of healthy part of vein and since vein size is so variable? If so, doesn't this increase vein damage/risk of rupture for smaller veins?
absolutely do not use one size fits all approach. Depends upon the initial diameter. Maybe we can get a 60-80% increase in IJV in most cases. !
we want to expand the vein up to but not more than it can tolerate without rupture. It is not an absolute but jugulars seem to tolerate 18-22mm stretch except when there is hypoplasia. Azygos seems to tolerate 6-10 mm well.
Do we have data on reduction of re-stenosis due to usage of larger balloons, or just Dr. Sinan's observations? I think some IR's in California are also using larger balloons too. Is it riskier?
Thanks!
no hard data yet, just personal testimony. But it makes sense which is the first step
Posted: Mon Dec 13, 2010 9:42 am
by drsclafani
CCSVIhusband wrote:
So, Dr., it's valves? Valves are the main CCSVI problem?
In the azygous I believe there are 3 valves (often malformed)?
and in the jugulars at the bottom?
the azygos often has no valves, it usually has one valve. Three valves are uncommon . The valve can be abnormal.
What about webs?
webs are very common in the azygos vein, probably more than the valve problems. Very difficult to detect, in my opinion.
Also ... it's 327 AM and you're posting away ... when do you sleep???
soon

one more ... can you speak briefly to elastic recoil? The process, just anything generally ... educate us a bit please!
let me think about another way to explain it. i think i can
Posted: Mon Dec 13, 2010 11:22 am
by Cece
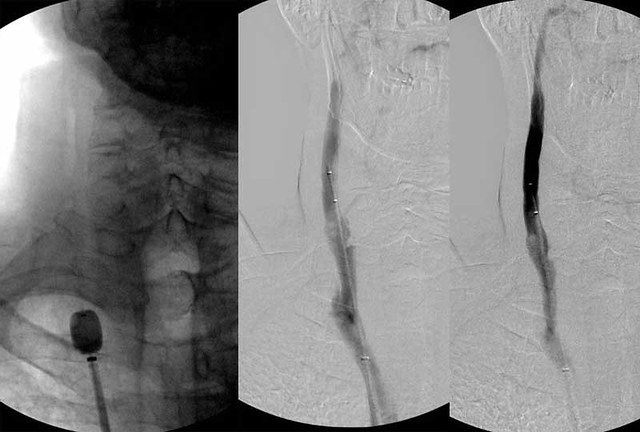
drsclafani wrote:So Finally a thrombectomy catheter was placed in there and further clot was stripped out. The final image looks better. you can still see the hypoplasia in the upper part of the vein. I just do not know how to deal with that yet..
Ok, I see you ARE taking questions.

That final image looks better than I would've thought likely. Kudos. Do you change the anticoagulation regimen or extend it past the three weeks, since there was already clotting occurring? Was the patient anticoagulated before the procedure? There might've been not much to lose at the start of this, but there's something to lose now....
Posted: Mon Dec 13, 2010 12:19 pm
by NZer1
Hi Dr, I have noticed that the vavles when opened are very complex (pathology studies). They appear to be quite a challenge when you look at how they attach and how they are situated to allow for vein enlargement and remain functional, almost a spiral where they attach.
Is it possible that these are going to in 'some' cases require removal as opposed to stretch to overcome their blocking effect. My thought is that at some point there will be indications which are best treated in curtain ways.
If the problem types were identified and some how their position recorded is it possible that some form of micro surgery could access and remove the dysfunctional value completely? In my mind it seems that some of these problem puppies may need to be removed rather than be an on going, on growing issue hanging in there. Not very technical explanation, but simple is good

Posted: Mon Dec 13, 2010 12:28 pm
by NZer1
Cece wrote:drsclafani wrote:So Finally a thrombectomy catheter was placed in there and further clot was stripped out. The final image looks better. you can still see the hypoplasia in the upper part of the vein. I just do not know how to deal with that yet..
Ok, I see you ARE taking questions.
That final image looks better than I would've thought likely. Kudos. Do you change the anticoagulation regimen or extend it past the three weeks, since there was already clotting occurring? Was the patient anticoagulated before the procedure? There might've been not much to lose at the start of this, but there's something to lose now....
To me this looks good above the deflated balloon in the RH photo, but I am very nervous about the look over the area below.
I would be wanting to understand what is happening with the shapes that are there and in particular understand the bulging areas, the one just below the balloon and the other with the dark spot in particular.
Question, the stretched valve, is there any indication what is happening with the remaining pieces of valve or the sides of the vein wall? I have the feeling this will be reason to not 'trust' that the problem is over.
sclafani asks a question
Posted: Mon Dec 13, 2010 5:58 pm
by drsclafani
are things heating up, or is it just the holidays
something seems to be building to me
Re: sclafani asks a question
Posted: Mon Dec 13, 2010 6:28 pm
by NZer1
drsclafani wrote:are things heating up, or is it just the holidays
something seems to be building to me
I'm a PwMS, got problems sensing things Dr. give us a bigger clue!

Posted: Mon Dec 13, 2010 6:30 pm
by Cece
Not sure what you mean...are you asking if your thread is heating up? Your thread is on fire!
Traditionally, forums die down a bit for holidays, although not when people make huge announcements on, oh, Thanksgiving, that sort of thing.
Posted: Mon Dec 13, 2010 6:47 pm
by NZer1
Hope its not a vein under duress! Is that what happened?
Posted: Mon Dec 13, 2010 7:07 pm
by CenterOfGravity
Sounds to me like something up his sleeve....
Posted: Mon Dec 13, 2010 7:54 pm
by NZer1
Whole foods, Vege diet can cause a build up ?
Posted: Tue Dec 14, 2010 4:22 am
by drsclafani
Cece wrote:drsclafani wrote:So Finally a thrombectomy catheter was placed in there and further clot was stripped out. The final image looks better. you can still see the hypoplasia in the upper part of the vein. I just do not know how to deal with that yet..
Ok, I see you ARE taking questions.
That final image looks better than I would've thought likely. Kudos. Do you change the anticoagulation regimen or extend it past the three weeks, since there was already clotting occurring? Was the patient anticoagulated before the procedure? There might've been not much to lose at the start of this, but there's something to lose now....
This patient was anticoagulated before getting on the procedural table. I will keep it that way for three weeks.
perhaps a second treatment will be warranted, perhaps more. We will wait until after the one month Doppler to review and make a recommendation to the patient.
yes, this was a bit better than i would have thought too.
it goes to show that the venogram in isolation cannot predict how the vessel will respond to the dilatation.
I am very curious to see whether that upper area of the vein will dilate now that there is better flow.