Page 370 of 557
Posted: Sat Jul 30, 2011 8:05 pm
by drsclafani
Cece wrote:HappyPoet wrote:drsclafani wrote:Perhaps the 16 mm balloon will be judged to be too small but i calculated that the 16 mm balloon is about 50% greater in surface area than the cross sectional area of these veins. I am dilating to 50-80% increase in cross sectional area measurement.
If a patient wanted a conservative procedure, is balloon sizing an area where a patient could ask for you to dilate only to a 50% increase in cross sectional area measurement as opposed to 80%?
To piggyback on this question, it could be asked more broadly: what changes would you make if a patient specifically requested a very conservative treatment?
i would do exactly what i am doing now
Posted: Sat Jul 30, 2011 8:06 pm
by drsclafani
Cece wrote:drsclafani wrote:Patient has previously been treated by a well known and respected interventionalist. The first treatment revealed a right sided stenosis that was treated with a 12 mm balloon. The left side was thought to be an insignificant stenosis. There were improvements in several symptom complexes. The symptoms gradually returned over the next couple of months.
A second procedure done a few months after the first showed that the right IJV was not restenosed, but the left IJV was felt to be significantly stenosed and was treated with a 14 mm balloon. Again with clinical improvements and yet again with gradual deterioration back to baseline.
This then might be the clinical profile of undertreatment? Although it might vary from patient to patient. Gradual deterioration of improvements.
or no improvements
Posted: Sat Jul 30, 2011 8:08 pm
by drsclafani
Cece wrote:drsclafani wrote:So I used the same 16 mm balloon to dilate the confluens of the right IJV.
A cost-saving measure? ;)
fortuitous
i look forward to the review of the number of balloons used per procedure.
s
Re: DrSclafani answers some questions
Posted: Sat Jul 30, 2011 8:11 pm
by drsclafani
tinajo wrote:Dear Dr. Sclafani,
I have a big decision to make and I am in need of your advice.
I recently had a doppler US in Arizona with Eric Feigenbutz. I basically have oversized, floppy valves/leaflets in my IVJ.
So, I was considering travel to NY to see you- however Dr. Makris is much closer and no flying.
My questions are:
Are your discoveries shared with the other AAC doctors?
especially dilation size and length and type of anti-coagulants.
If I am treated now- and plan on staying around another 40 + years will my veins be able to hold up to future tune ups or do I risk damaging them for future improvements in treatment. I realize this is a difficult question- but I would like your thoughts on this.
Thank you for everything- I can't truly express the gratitude I feel for your willingness to make yourself available to us- I was having such anxiety over this until I discovered you on TIMS. You made it all so real to me.
Best Regards,
Tina
We do share techniques and ideas. However each physician is his own practice and each physician ultimately decides how he will treat
moreover, the other centers currently do not use IVUS so their practices are somewhat different from mine
Re: IVUS Imaging
Posted: Sat Jul 30, 2011 9:10 pm
by NHE
Hi Dr. Sclafani,
I have become interested in interpreting IVUS images especially after reading the book 'IVUS Made Easy'.
You recently posted the image below.
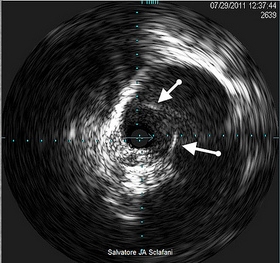
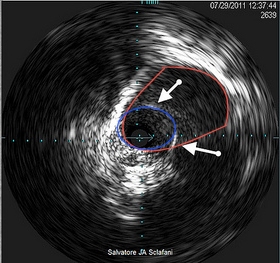
How would you describe the cross sectional patency of this vein? In the image below, would it be the area outlined in blue or the area outlined in red? Or, perhaps some other area?
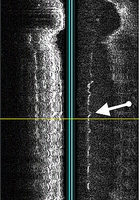
In addition, in the longitudinal compilation image, would it be correct to interpret the white line which seems to appear in the middle of the vein as a membrane splitting the vein in two? Or, is this the inner intimal wall of the vein in this section with the vein lumen to the left of the white echogenic line? If neither is correct, how do you interpret this line?
Thanks, NHE
Re: IVUS Imaging
Posted: Sun Jul 31, 2011 6:33 am
by drsclafani
NHE wrote:Hi Dr. Sclafani,
I have become interested in interpreting IVUS images especially after reading the book 'IVUS Made Easy'.
EASY??? Took me a year to figure this stuff out and i am still interpreting what i am seeing.
NHE wrote:You recently posted the image below.
How would you describe the cross sectional patency of this vein? In the image below, would it be the area outlined in blue or the area outlined in red? Or, perhaps some other area?
cross sectional area in red divided by cross sectional area in blue equals percentage of stenosis. The red circle is the lumen of the vein that is continuous with the vein above from which blood flows. The valve is narrowed within the larger vein, like a funnel. that is why you can see the vein fully and see the narrowed valve within it, but the narrowed area becomes the bottleneck. is that clear?
nhe wrote:
In addition, in the longitudinal compilation image, would it be correct to interpret the white line which seems to appear in the middle of the vein as a membrane splitting the vein in two? Or, is this the inner intimal wall of the vein in this section with the vein lumen to the left of the white echogenic line? If neither is correct, how do you interpret this line?
Thanks, NHE
The probe is in the middle. sound reflects off the walls. on the left is echo off the wall of the vein. To the right first there is echo off the stenotic valve (the white line in the middle). Further to the right is echo off the opposite wall of the vein.
Is that clearer?
Posted: Sun Jul 31, 2011 7:34 am
by Cece
I agree with not lurking, it is more fun with more people involved.
'Ivus Made Easy' still cracks me up. And I will have to get a copy.
For the most part the vein above the stenosis is usually smaller than below the stenosis.
Do you know why the vein above the stenosis is smaller than below the stenosis?
Posted: Sun Jul 31, 2011 8:05 am
by drsclafani
Cece wrote:I agree with not lurking, it is more fun with more people involved.
'Ivus Made Easy' still cracks me up. And I will have to get a copy.
For the most part the vein above the stenosis is usually smaller than below the stenosis.
Do you know why the vein above the stenosis is smaller than below the stenosis?
Easy, since the stenosis is usually at the valve, the vein below the valve includes the flow of the subclavian vein too. this vein, called inominate vein, is usually larger than the jugular.
however one of the reactions to obstruction is dilation of the vein ABOVE the stenosis. So sometimes this dilation is so large that it is better to put the balloon mostly above the stenosis to avoid injuring normal vein.
Posted: Sun Jul 31, 2011 8:25 am
by HappyPoet
DrS, in my thank-you post for answering all my questions, I forgot to say thank you which is, when forgotten, undeniably unfortunate, utterly uncouth, unquestionably unforgivable, unbelievably unprofessional, and ultimately unconscionable for a universally ubiquitous, uniform, unconditional, and unambiguous utterance that is unequivocally understood when used.
THANK YOU, DrS, for answering all my questions.  [NotJ, u=19]
[NotJ, u=19]
Posted: Sun Jul 31, 2011 9:05 am
by pklittle
HappyPoet is uber-talented.
I thought
NHE was serious about a book called "Ivus Made Easy". DUH

Posted: Sun Jul 31, 2011 9:59 am
by Cece
He is serious!
http://www.amazon.com/IVUS-Made-Easy-Pa ... 1841845957
the 7th edition IVUS Pocket Guide might also come in handy. 'Fits in the palm of your hand!"
http://tinyurl.com/3d4eote
Posted: Sun Jul 31, 2011 10:00 am
by sou
One question (that may have already be answered, but missed):
At the top of the sagital reconstruction, the vein looks completely anomalous. Is this because the probe as travelling inside the vein found turns in its way, but had no way of "knowing" they are turns, so it "thought" that it is an anomalous straight wall?
(I hope what I have written is understandable. I find it difficult, too...)
Posted: Sun Jul 31, 2011 10:52 am
by Cece
drsclafani wrote:HappyPoet wrote:
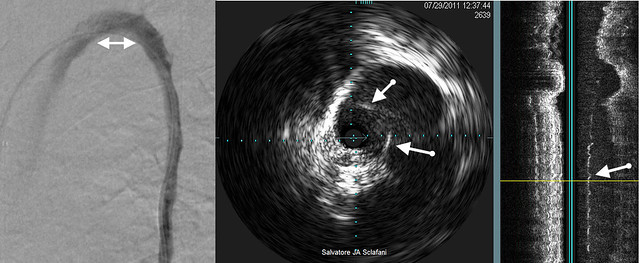
This shows the value of IVUS.
I honestly don't see anything on the sagital reconstruction where the arrow is pointing near the thin, green horizontal line. What does the large shift in signal represent far above the arrow?
the large shift represents movement of the tissue during normal breathing,and pulsations.
I didn't know that. That's why we never talk about that, because it's just movement.
drsclafani wrote:i would consider the green line to be vertical. It represents the plane of the ivus device. to the right of the green lines one sees some white longitudinal speckles. There represent sound reflections off the narrowed valvular area.
Do you see it now, HappyPoet? Right where the arrow is pointing, there is a white vertical squiggly line?
The rest of the valve does not show up but it is there blocking flow; what shows up is that white line which is the thickened edge of the valve leaflets. It shows up because it is thickened. Echo doppler does not show thin, only thick. Thick things in the middle of our veins are probably blocking the flow. The walls of the vein themselves are thick, which is why we see them too.
btw it worked to have your questions all in one post, it was easy to see which part of the case you were asking about, I wouldn't worry about that. You rocked it.
Re: DrSclafani answers some questions
Posted: Sun Jul 31, 2011 11:47 am
by Cece
drsclafani wrote:tinajo wrote:Dear Dr. Sclafani,
I have a big decision to make and I am in need of your advice.
I recently had a doppler US in Arizona with Eric Feigenbutz. I basically have oversized, floppy valves/leaflets in my IVJ.
So, I was considering travel to NY to see you- however Dr. Makris is much closer and no flying.
My questions are:
Are your discoveries shared with the other AAC doctors?
especially dilation size and length and type of anti-coagulants.
If I am treated now- and plan on staying around another 40 + years will my veins be able to hold up to future tune ups or do I risk damaging them for future improvements in treatment. I realize this is a difficult question- but I would like your thoughts on this.
Thank you for everything- I can't truly express the gratitude I feel for your willingness to make yourself available to us- I was having such anxiety over this until I discovered you on TIMS. You made it all so real to me.
Best Regards,
Tina
We do share techniques and ideas. However each physician is his own practice and each physician ultimately decides how he will treat
moreover, the other centers currently do not use IVUS so their practices are somewhat different from mine
There has been a lot of talk lately about if multiple procedures are safe or should be avoided. Dr. Arata, who uses larger balloons and higher pressures, and Dr. Siskin, who is more gentle on the veins, have both concluded that caution is warranted before doing multiple procedures. Dr. Sclafani's answer has been that we do not yet know what the limit is. It may be unlimited. There were some nuances to his answer, it's a page or two back, it was also discussed at the AAC Patient Day.
Dr. Sclafani's strategy of using IVUS to measure the vein is more precise than other doctors' methods of eyeballing it from the flouroscopy image. Dr. Sclafani and Dr. Cumming both have shown us examples where the oval-shaped vein has a significantly different measurement when done by IVUS than when done by eyeballing. Being precise about the measurement is important because the measurement is used to choose balloon size. Too large of a balloon may damage the vein. So, his strategy may be better than that of other doctors at protecting the vein from damage, which would allow for more future procedures.
There needs to be clinical research done before we know any of this for certain. Other doctors do not discount that IVUS adds extra information, the debate is whether that extra information is worth the extra cost. When it was my own veins at stake, yes, I found it to be worth the extra cost.
I know you asked for Dr. Sclafani's thoughts and, for this portion of the question, what you got was Cece's. Sorry about that.
Posted: Sun Jul 31, 2011 12:30 pm
by 1eye
If a vein is shaped like an oval it has two diameters. Which one are you using for the balloon size, or is it somewhere in between? I suppose there is a mathematical way of calculating the circumference or the radius it would have if it were round. Are you getting that finicky about it? If so, good!