Page 396 of 557
Re: DrSclafani answers some questions
Posted: Mon Oct 03, 2011 8:50 pm
by drsclafani
Cece wrote:drsclafani wrote:This data is also being reviewed. Preliminarily: venography looks normal in 40 per cent of the azygous valvular stenoses found by IVUS
Very nice!
You've seen the abstract on IVUS presented at CIRSE, with a very small sample size but similar findings that IVUS was able to show stenoses not seen on venography?
http://www.thisisms.com/forum/chronic-c ... ml#p175921
Another side of the coin is if there are any cases that are the opposite, where venography shows an apparent stenosis that, upon using IVUS, is not a real one. And you must be tabulating how often the venography looks normal in the jugulars too but IVUS reveals a stenosis. Is this less common in the jugulars than in the azygous?
first, understand that venography usually is performed before IVUS. Thus while venography is done blinded to results of IVUS, the opposite is not true yet. That will be food for another study. The goal here is to determine whether there are valvular, web, septal pathology that is not detected by venography that can be seen by IVUS.
But to answer your comment, yes, there are instances of abnormal venograms and unremarkable IVUS exams.
I would not suggest that either ivus or venography should be considered the gold standard by itself
Re: DrSclafani answers some questions
Posted: Mon Oct 03, 2011 8:53 pm
by drsclafani
Cece wrote:
What I am taking from all of this is that, instead of pelvic congestion syndrome affecting the cerebrospinal drainage, it is the messed-up cerebrospinal drainage that has affected the pelvic veins.
Correct
Re: DrSclafani answers some questions
Posted: Mon Oct 03, 2011 10:09 pm
by NHE
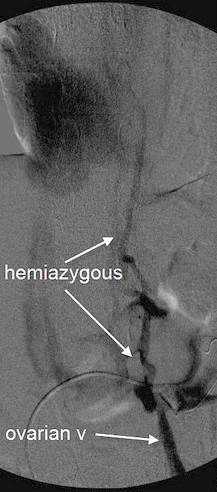
Cece wrote:Now that I've got the layout down, wow, that is an extreme change from the first to the second image. Once the stent is in, nothing lights up but the renal vein and the IVC.
If you lighten the image by doing a gamma correction, it appears that there is a stent in the first frame of the image.
NHE
Re: DrSclafani answers some questions
Posted: Tue Oct 04, 2011 7:09 am
by Cece
NHE wrote:Cece wrote:Now that I've got the layout down, wow, that is an extreme change from the first to the second image. Once the stent is in, nothing lights up but the renal vein and the IVC.
If you lighten the image by doing a gamma correction, it appears that there is a stent in the first frame of the image.
NHE
I don't think this is right. Dr. Sclafani said:
drsclafani wrote:in the middle image there is a stent. that is why you are not seeing the hemiazygous and the ascending lumbar vein
In the first image we are seeing the hemiazygous and the ovarian vein, therefore no stent yet, in my interpretation.
Re: DrSclafani answers some questions
Posted: Tue Oct 04, 2011 4:04 pm
by THEGREEKFROMTHED
Mortadella. Hope u r well. Prominent dr in my area performing the good reamings but enters right groin and does not anticoagulate!! Please your deepest intermost thoughts. Please seriously tell me your opinion. Your man. The greek
Re: DrSclafani answers some questions
Posted: Wed Oct 05, 2011 8:10 am
by drsclafani
NHE wrote:Cece wrote:Now that I've got the layout down, wow, that is an extreme change from the first to the second image. Once the stent is in, nothing lights up but the renal vein and the IVC.
If you lighten the image by doing a gamma correction, it appears that there is a stent in the first frame of the image.
NHE
There is NO stent in the first image to the left. the stent is in the middle image.
Re: DrSclafani answers some questions
Posted: Wed Oct 05, 2011 8:16 am
by drsclafani
THEGREEKFROMTHED wrote:Mortadella. Hope u r well. Prominent dr in my area performing the good reamings but enters right groin and does not anticoagulate!! Please your deepest intermost thoughts. Please seriously tell me your opinion. Your man. The greek
Ask him to read Dr Zamboni's paper. A complete exam by zamboni protocol includes left iliac venogram, left renal venogram and left ascending lumbar venogram. I follow these recommendations as my standard. I also place catheter or guidewire in the dural sinus to assure that i have imaged the ENTIRE internal jugular vein.
With regard to anticoagulation, I do think there is always a risk of thrombus formation when you damage the intima which is a standard component of venoplasty or valvuloplasty. Short term anticoagulation with a thrombin a inhibitor and antiplatelet therapy with aspirin for a month seems prudent.
I remind you of the era of thromboses that occured in 2010 and early 2011. Thrombus does occur and we need to avoid permanent thrombosis of the vein.
Wish him luck for me.
Re: DrSclafani answers some questions
Posted: Wed Oct 05, 2011 9:20 pm
by beerduff
http://www.facebook.com/l.php?u=http%3A ... =gAQD4loYw
Dr Sclafani
What is your expert opinion on the link?
Have you also noticed trauma to the cervical spine.
It would be very interesting to find out if patients had any recollection of serious trauma in the past.
Is there way to go back on all the many scans you have undertaken to see if there is a link.
I have asked my wife, she does not remember having any problems previously.
I will try and find out from her mother on the weekend.
Re: DrSclafani answers some questions
Posted: Fri Oct 07, 2011 6:53 am
by THEGREEKFROMTHED
Morty,
I hope you didnt pull any neck muscles watching Detroit Tiger Homeruns go over your head. RUmor has it you were sitting in shallow right? My deepest sympathys to you and A-ROd 0-4 yesterday striking out for the last out. Tissues anyone??
Greek from the "D"
Re: DrSclafani answers some questions
Posted: Sat Oct 08, 2011 4:52 pm
by drsclafani
beerduff wrote:http://www.facebook.com/l.php?u=http%3A ... =gAQD4loYw
Dr Sclafani
What is your expert opinion on the link?
Have you also noticed trauma to the cervical spine.
It would be very interesting to find out if patients had any recollection of serious trauma in the past.
Is there way to go back on all the many scans you have undertaken to see if there is a link.
I have asked my wife, she does not remember having any problems previously.
I will try and find out from her mother on the weekend.
It is an interesting paper but the results are a bit different than my experience.
Below is a copy of the first page of my three page medical questionaire that i send to patients who inquire about treatment to my email,
ccsviliberation@gmail.com. I use the questionaire to screen for unusual circumstances that require more in-depth discussion before scheduling PwMS for treatment in my office.
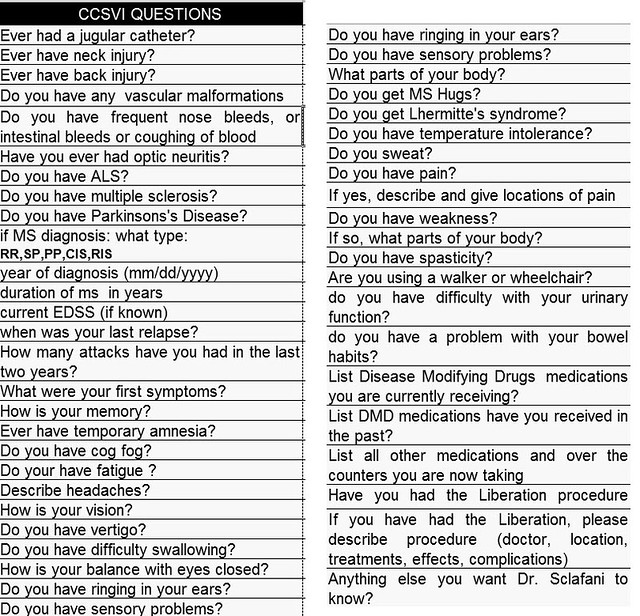
I have always considered prior trauma as an association with CCSVI since the first patient I treated. You will note that the second and third questions ask about trauma of the back and the neck. Since day 1!
However, I have not noted any association between prior neck trauma and MS. the question is usually answered by stating that there has been no prior neck trauma. A positive history is present in less than 5% of my patients. Even in these patients, i did not detect any significant findings in the spine or the veins adjacent to the spine in the venograms. Granted I am not looking at CSF flow.
Based upon this data, i do not see a correlation.
I know Ray Damadian for many years. In my opinion (not that anyone cares) he deserved to receive a Nobel Prize for his creation of the first MRI unit. He is always thinking outside the box.
I remember this wild scientist coming into the xray reading room at the hospital when i was a resident in training in 1975. He asked whether i agreed with him that an early MRI image showed evidence of a cancer. I had no idea what he was speaking about andI had no idea how to interpret the first cancer MRI image.
I will call Ray and speak about this when I get a chance.
Best wishes
DrS
Re: DrSclafani answers some questions
Posted: Sat Oct 08, 2011 4:57 pm
by drsclafani
THEGREEKFROMTHED wrote:Morty,
I hope you didnt pull any neck muscles watching Detroit Tiger Homeruns go over your head. RUmor has it you were sitting in shallow right? My deepest sympathys to you and A-ROd 0-4 yesterday striking out for the last out. Tissues anyone??
Greek from the "D"
Greek I hate you
i hadnt taken my second bit of my foot long hot dog before two Detroit homers had offended the House that Ruth did not build, but would have enjoyed if he were alive. They were less than ten feet farther than the two shots that just fell short for the yanks.
o, well....i have lived through enough world championships in my life, probably around fifteen. Not bad for a kid from brooklyn whose first team abandoned him at age of 11.
Re: DrSclafani answers some questions
Posted: Sun Oct 09, 2011 11:08 am
by drsclafani
The next case i will share is a story of two people, mother and son.
Mother with secondary progressive MS for thirty years resulting in in weakness and spasticity in the lower extremities and bladder, but she is mobile. Chronic fatigue, temperature intolerance and right sided deafness were also present. She underwent venoplasty in April by another interventionalist with improvements to that lasted only three weeks.
Her 34 year old son was diagnosed with multiple sclerosis at age 31. His course has been unrelenting. Severe cerebellar intention tremors have been incapacitating. Weakness, choking, and no response to medications.
Mother received angioplasty once. Son had angioplasty twice. Both had angioplasty of right and left internal jugular veins and azygous vein. Both had clinical improvements in spasticity and weakness. Even the son's tremors markedly decreased. Unfortunately both patients' improvements were very short lived.
I was struck by the similarity of the venographic appearances and the dissimilar clinical presentations.
My study showed that the azygous and right internal jugular vein angioplasties were well maintained with no stenoses, or valvular immobility.
This is a comparison of each patients's left internal jugular veins:

Re: DrSclafani answers some questions
Posted: Sun Oct 09, 2011 2:04 pm
by Cece
drsclafani wrote:Her 34 year old son was diagnosed with multiple sclerosis at age 31. His course has been unrelenting. Severe cerebellar intention tremors have been incapacitating. Weakness, choking, and no response to medications.
As a mom, this is the worst fear.

This is a comparison of each patients's left internal jugular veins:
You can see the contrast refluxing at the top of the jugular into collateral veins in both images.
The image on the left looks like it has a narrowing near the area of the valves.
The image on the right shows a more complicated flow situation, with apparent stenoses both lower down and up at J3.
Was the prior angioplasty at the area of the valves? Was this J3 stenosis observed and/or treated during the prior treatments? Had IVUS ever been used on these patients? Or the renal or iliac veins checked? I like stories with happy endings....
Did you find a possible explanation as to why patients with similar venograms would have such dissimilar courses?
Re: DrSclafani answers some questions
Posted: Sun Oct 09, 2011 3:59 pm
by THEGREEKFROMTHED
And a dads
Re: DrSclafani answers some questions
Posted: Mon Oct 10, 2011 11:32 am
by pelopidas
"Did you find a possible explanation as to why patients with similar venograms would have such dissimilar courses?"
also, why patients with (as far as we know) dissimilar venograms would have similar courses?
i'm looking forward to the rest of the story of this family case