NZer1 wrote:IVUS, why guess?
Seems to me that visually we are seeing areas of interest only, follow the clues/hints and IVUS to remove doubt!
As you wish. my goal was to illustrate that stenoses are present even in the absence of direct evidence of stenosis by venography.

i think the image speak for themselves. IVUS shows immobile valves treated by 18 mm angioplasty to 8 ATM.
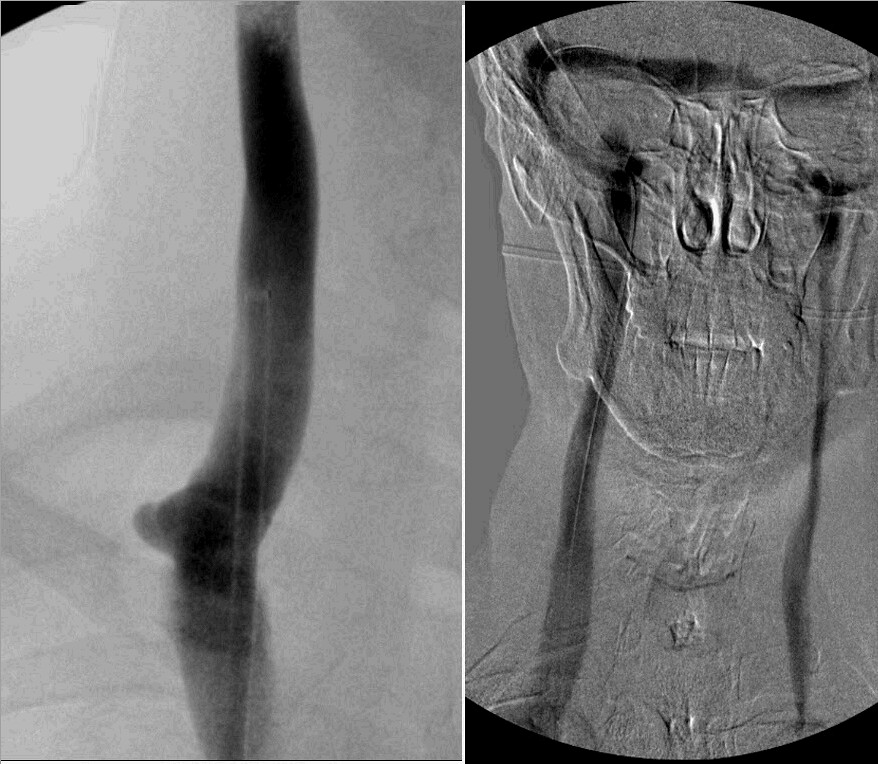
The left jugular venogram , as you could see from the right sided venogram reflux, is small in the upper area of the neck. Further it is narrowed even more in the lower neck. This valve was quite tight.
The initial work was done in the lower jugular vein. I wanted to assure myself that the upper narrowing wasn't just a physiological narrowing caused by the lower stenosis.
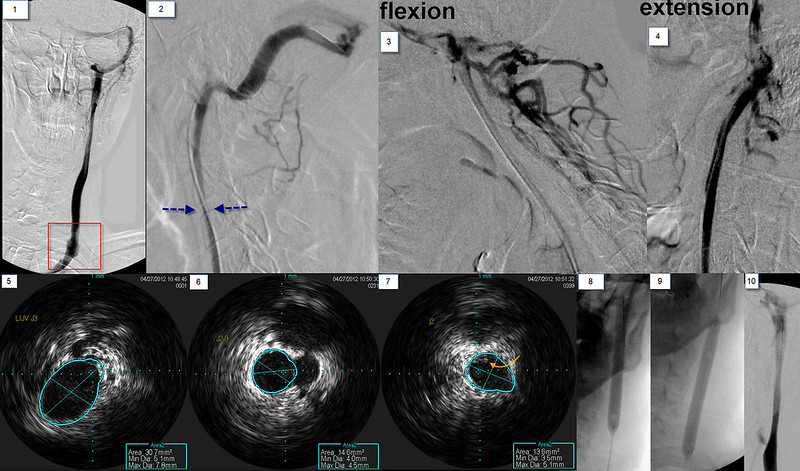
There is a stenosis at the confluens with the subclavian vein (red arrows). there is reflux into the anterior jugular vein. images 3,4,5,6 show the thickened leaflets (white arrows) resulting in a 67% stenosis of this hypoplastic vein. These thicked areas are better seen in image 7. A 14 mm balloon was inflated to open this valve. The post angioplasty imag shows improvement in luminal diameter and no visualization of the anterior jugular vein.
The upper jugular vein was more challenging. in image 2 you can see the narrowing of the upper internal jugular vein (blue arrows). By flexing the neck, the vein is completely occluded with a lot of filling of posterior cervical veins connecting to emissary veins. In extension, the lumen looks great!
The three ivus images show the dimensions of the vein. a 7mm vein decreased to a 4mm balloon lower down and it remained that size for a while. So, is this a hypoplasia? in image 7 the orange arrown points to intraluminal material. That resembles thrombus to me. Perhaps this is all a recanalized old occlusion of the IJV? or the results of an inflammatory process? The patient said he had many throat infections while growing up. Could this be the result of an infectious process? Any way, i did angioplasty with a long 8 mm balloon. REsults seem to show some improvements
Finally, the azygous vein, the brachiocephalic veins, the left renal vein, the left ascending lumbar vein, the left common and exernal iliac veins were all normal .
On the table the patient said that his pins and needles were gone and he started to move his paralyzed ankle. Said vision might be a bit clearer too.
In recovery room i reevaluated him. Strength in his paralyzed ankle was normal and equal to the other side. numbness in both hands and feet had resolved. unlike the day before, he could feel the pain of a n eedle in his foot and fingers. Rhomberg;s test was normal, he could stand with his eyes closed.,
He came out of the dressing room carrying his cane, not using it. Amazing result.
The next day he went on a two block walk without his cane.