Page 461 of 557
Re: DrSclafani answers some questions
Posted: Thu May 31, 2012 6:29 pm
by Cece
drsclafani wrote:The challenging part is that there is going to be an overlap of symptoms caused by ccsvi and the symptoms caused by MS. I thinkm that is why it is so difficult to predict response.
An overlap. I haven't heard it described that way before. Makes perfect sense.
(Overlap meaning we might have fatigue caused by MS and/or we might have fatigue caused by CCSVI syndrome. We might have limb weakness caused by MS and/or limb weakness caused by CCSVI syndrome. And you only sort out which is which when you see which symptoms disappear after successful CCSVI treatment, and which remain.)
Re: DrSclafani answers some questions
Posted: Fri Jun 01, 2012 10:35 am
by Thekla
I like the overlap description. I think it fits well. But I think there are probably multiple overlaps, hence some get great symptom relief with diet, others with atlas balance, others with ccsvi and others possibly some other treatment.
Re: DrSclafani answers some questions
Posted: Fri Jun 01, 2012 7:45 pm
by drsclafani
Cece wrote:drsclafani wrote:The challenging part is that there is going to be an overlap of symptoms caused by ccsvi and the symptoms caused by MS. I thinkm that is why it is so difficult to predict response.
An overlap. I haven't heard it described that way before. Makes perfect sense.
(Overlap meaning we might have fatigue caused by MS and/or we might have fatigue caused by CCSVI syndrome. We might have limb weakness caused by MS and/or limb weakness caused by CCSVI syndrome. And you only sort out which is which when you see which symptoms disappear after successful CCSVI treatment, and which remain.)
I posit that you might have symptoms of weakness from both ccsvi and ms, and get some varied response.
obviously conjecture. I am just trying to figure out a rationale why some patients have amazing improvements and others do not.
if we could ever get buy in by colleagues, there is much to think about.
Re: DrSclafani answers some questions
Posted: Sat Jun 02, 2012 2:48 am
by MarkW
drsclafani wrote:Cece wrote:drsclafani wrote:The challenging part is that there is going to be an overlap of symptoms caused by ccsvi and the symptoms caused by MS. I thinkm that is why it is so difficult to predict response.
An overlap. I haven't heard it described that way before. Makes perfect sense.
(Overlap meaning we might have fatigue caused by MS and/or we might have fatigue caused by CCSVI syndrome. We might have limb weakness caused by MS and/or limb weakness caused by CCSVI syndrome. And you only sort out which is which when you see which symptoms disappear after successful CCSVI treatment, and which remain.)
I posit that you might have symptoms of weakness from both ccsvi and ms, and get some varied response.
obviously conjecture. I am just trying to figure out a rationale why some patients have amazing improvements and others do not.
if we could ever get buy in by colleagues, there is much to think about.
An interesting discussion but please focus on giving safe effective therapy for CCSVI syndrome and getting other IRs to follow this. After 50 years of massive spending on MS research, Neuros cannot be certain of the causative factors of MS, so I do not give IRs much chance in the next few years, even if the Neuros play ball.
Kind regards,
MarkW
Re: DrSclafani answers some questions
Posted: Sat Jun 02, 2012 9:29 am
by Cece
Buy-in by the neurologists will eventually happen, unless the results from RCTs are shockingly different than expected.
The degree of echogenicity of the valve is not great but sufficient to make it perceptible. I will find a case of long standing CCSVI in a patient with more than 20 years of MS. The difference is striking.
any image to share?
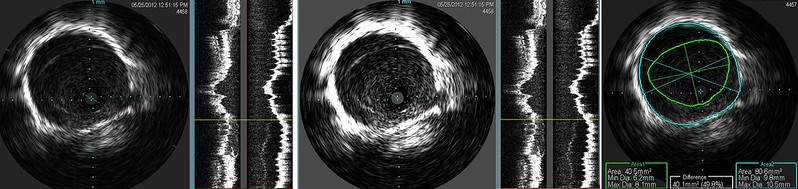
Again IVUS is not equivocal in this case. I showed the same image in two different brightness/contrast levels to illustrate how subtle it can be. Image too dark and it can very difficult to see the immobile valve. Looking at this abnormality, i was not impressed by the degree of stenosis on visual terms. But the IVUS calculation show this to be just about a 50% stenosis. More than the eye can tell.
Definitely easier to see in the second image.
If residual valve material is a frequent cause of restenosis, could the thickness of the valve as seen on IVUS be predictive of how much residual valve material will remain and whether restenosis will occur?
Such a case illustrates how even the accepted Gold Standard may miss stenoses in apparently normal looking venograms. Venography is less than perfect because the disease is not generally of the vein itself. But rather of the valve which is much better visualized by IVUS.
Re: DrSclafani answers some questions
Posted: Sat Jun 02, 2012 7:10 pm
by drsclafani
An interesting discussion but please focus on giving safe effective therapy for CCSVI syndrome and getting other IRs to follow this. After 50 years of massive spending on MS research, Neuros cannot be certain of the causative factors of MS, so I do not give IRs much chance in the next few years, even if the Neuros play ball.
Kind regards,
MarkW
These are very important factors in providing safe and effective therapy. Frankly. We need to try to determine which patients will benefit and which will be harmed by this therapy. And I think it will be delayed by the lack of collaboration.
This discussion has nothing to do with the cause of ms but with assessing the manifestations of both ms and ccsvi. One of the keys will be the symptoms
Re: DrSclafani answers some questions
Posted: Sat Jun 02, 2012 10:15 pm
by NZer1
drsclafani wrote:
An interesting discussion but please focus on giving safe effective therapy for CCSVI syndrome and getting other IRs to follow this. After 50 years of massive spending on MS research, Neuros cannot be certain of the causative factors of MS, so I do not give IRs much chance in the next few years, even if the Neuros play ball.
Kind regards,
MarkW
These are very important factors in providing safe and effective therapy. Frankly. We need to try to determine which patients will benefit and which will be harmed by this therapy. And I think it will be delayed by the lack of collaboration.
This discussion has nothing to do with the cause of ms but with assessing the manifestations of both ms and ccsvi. One of the keys will be the symptoms
Totally agree Dr S.
One of the key points was made above by Cece I think. The reason that PwMS with the episodic form of MS are a case in point. The reason for a rapid loss of motor or sensory function has never been researched. It is one of the same factors in CCSVI (PTA with IVUS) Treatment that are of HUGE learning.
I asked on the main board a long time ago about the timing of the episodes and got little response that would have given any understanding at all.
The way that the episodes come on and then pass with sometimes residual losses is so similar to the PTA outcome that it is screaming for a group or several groups of interested researchers to make a name for them selves.
And again the changes in PPMS people is another reason for the PTA outcomes to be of incredible interest if there was people interested in ill Health causes.
It's sad there are only the few of us on this board that are passionate about life.
Regards all,
Nigel
Re: DrSclafani answers some questions
Posted: Sun Jun 03, 2012 9:03 am
by 1eye
Cece, elsewhere on ThisIsMS wrote:Subject: Dr. Berkoff on why UCC might work as a CCSVI treatment
...
Greg Berkoff, DC…one chiropractic Perspective
Upper cervical spine manipulation…is it a viable treatment option?
If upper cervical spine manipulation does help with ms then CCSVI might give a reason for why it works.
thereS a network of veins in, and around the 1st cervical vertebra. The vertebral plexus works selectively when we are upright
verterbral system is just as important as the internal jugular system.
All the veterbral veins develop in the upper cervical vertabra
Manual traction which can be sustained can provide decompression.
Looked at 1 pt and 4 normals to see if traction can increase flow. Traction applied before, MR venogram, and after venogram
Flow increases after traction
Pt with MS…flow -7.02 ,after traction -9.24 almost a 30% increase of flow(below 8 is abnormal)
Tractioning of the cervical spine may be a viable treatment for ccsvi
I believe I read E.B.White had a device for manual head self-traction which consisted of a helmet-like affair with a rope attached to it, which you could throw over a barn rafter. Sounds like a reason to be careful; you'd in all probability have enough rope to hang yourself.
Maybe not such a bad idea. I did a fairly hard neck compression shortly before I was diagnosed, when I was trying to get some Christmas lights off a tree and fell off the top of a six (eight?) foot ladder onto my backside.
Maybe vertebrals is why PTA sometimes doesn't work, or even only partly, since we can't balloon vertebrals?. If we could combine treatment by PTA with something for that -- traction?
Re: DrSclafani answers some questions
Posted: Sun Jun 03, 2012 11:24 am
by drsclafani
mo_en wrote:Great presentation Dr S!
Dr. Brenda Banwell is doing an ultrasound study on children with MS. If early CCSVI is difficult to trace by venography, i suspect it will be even harder to do with ultrasound. Do you agree?
Actually, i think it may be difficult to see CCSVI in children by all methodologies as i believe that the thickness of the valve leaflets may be too thin. However, i havent studied any children with ultrasound or IVUS.
If nothing is seen, will the conclusion be that ccsvi doesnt exist or that it is not visible?
mo-en wrote:To the questions:
1.
drsclafani wrote:but becamse exacerbation free while taking natalizumab (tysabri).
Do you think that Tysabri may act by reducing CCSVI severity? It's supposed to prevent T cells from adhering to the vein walls. Could this action be anticoagulant and allow a swift blood flow through the immobile valves?
2. Does blood flow speed influence the way a vein is opacified by contrast media? Is it possible that venograms of problematic veins look normal because blood speed is low and contrast particles have time to surround the valves? Have you noticed (measured?) differences in blood speed between patients and healthy controls?
#1 I do not know of any anticoagulant effects of natalizumab. I am not an MS specialist, but i am a vascular specialist and I would not say that anticoagulants increase speed of blood flow in general.
#2. I have noted decreased flow in patients with ccsvi compared to healthy control, the control being retrospective, namely evaluation of young men sustaining gunshot wounds of the neck, receiving arteriograms that show the venous phase . But more to the point, i have found that the more diminished the flow is, the easier it is to see these stenoses
Re: DrSclafani answers some questions
Posted: Sun Jun 03, 2012 11:26 am
by drsclafani
NZer1 wrote:drsclafani wrote:
An interesting discussion but please focus on giving safe effective therapy for CCSVI syndrome and getting other IRs to follow this. After 50 years of massive spending on MS research, Neuros cannot be certain of the causative factors of MS, so I do not give IRs much chance in the next few years, even if the Neuros play ball.
Kind regards,
MarkW
These are very important factors in providing safe and effective therapy. Frankly. We need to try to determine which patients will benefit and which will be harmed by this therapy. And I think it will be delayed by the lack of collaboration.
This discussion has nothing to do with the cause of ms but with assessing the manifestations of both ms and ccsvi. One of the keys will be the symptoms
Totally agree Dr S.
One of the key points was made above by Cece I think. The reason that PwMS with the episodic form of MS are a case in point. The reason for a rapid loss of motor or sensory function has never been researched. It is one of the same factors in CCSVI (PTA with IVUS) Treatment that are of HUGE learning.
I asked on the main board a long time ago about the timing of the episodes and got little response that would have given any understanding at all.
The way that the episodes come on and then pass with sometimes residual losses is so similar to the PTA outcome that it is screaming for a group or several groups of interested researchers to make a name for them selves.
And again the changes in PPMS people is another reason for the PTA outcomes to be of incredible interest if there was people interested in ill Health causes.
It's sad there are only the few of us on this board that are passionate about life.
Regards all,
Nigel
There are many people on this board that are passionate about life. Many just choose to read rather than write
Re: DrSclafani answers some questions
Posted: Sun Jun 03, 2012 1:04 pm
by Cece
1eye wrote:Maybe vertebrals is why PTA sometimes doesn't work, or even only partly, since we can't balloon vertebrals?
Remember this case? I think the threshold to choose to balloon a vert is higher, because there's no research on it and the verts are not the major routes like the internal jugulars, but it is worth researching and stetching the boundary in this direction, carefully, and for patients such as this one with an occluded jugular and an as-seen-on-IVUS bad valve in the vert.

drsclafani wrote:here you go, cece.
This is my first IVUS of a vertebral vein. The medical necessity for this IVUS was the fact that the internal jugular vein in J3 had long standing occlusion secondary to an overly aggressive angioplasty of a phasic compression of the IJV as it crosses the second vertebra. I saw some abnormality on the prior venogram and wanted to confirm my impression from the venogram that the vertebral had a valve and that it was thickened. I have read that the vertebral vein is valveless, but i think that is incorrect urban legend.
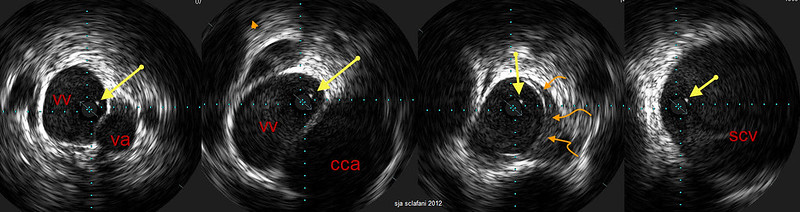
Four images
left: highest level before it turns into a vertebral plexus, which accounts for the tangles at the top of the venogram. this is in the bony canal with vertebral artery and vein nicely visible. on all four images one sees this echogenic dot (yellow arrows). I am thinking this is a web.
left middle: The vertebral artery is no longer seen. The larger common carotid artery is adjacent to this
right middle. Closer to the chest one sees the thickened valve that is immobile (curved orange arrows)
Right The vein is now entering the subclavian vein.
I performed a delicate vertebral vein angioplasty because the left IJV was occluded and not functioning.
http://www.thisisms.com/forum/chronic-c ... ml#p188661
That white dot (yellow arrows) is still awfully mysterious. It's hard to know if or how much a web affects flow. It is present throughout the vein.
Re: DrSclafani answers some questions
Posted: Sun Jun 03, 2012 4:33 pm
by msfire
Hi Doc, I'm sure this question has been asked before so I will apologize now for asking the same question again.
When you did the work on me last August my issues were the valves and the leaflets. Is there a procedure that would eliminate/remove the leaflets if they continue to cause restricted flow?
Thanks
Re: DrSclafani answers some questions
Posted: Sun Jun 03, 2012 6:41 pm
by newlywed4ever
drsclafani wrote:There are many people on this board that are passionate about life. Many just choose to read rather than write
You took the words right out of my mouth.
Re: DrSclafani answers some questions
Posted: Sun Jun 03, 2012 7:07 pm
by HFogerty
Certainly 794447 views to date says it all

Re: DrSclafani answers some questions
Posted: Sun Jun 03, 2012 7:15 pm
by tiltawhirl
HFogerty wrote:Certainly 794447 views to date says it all
Indeed.
tilt