Page 464 of 557
Re: DrSclafani answers some questions
Posted: Tue Jun 26, 2012 10:12 pm
by NZer1
Cece are you meaning to say your interested to know what the good Dr has been up to, and even more interested to hear what his mind is finding?
I know I am!
Re: DrSclafani answers some questions
Posted: Wed Jun 27, 2012 9:43 am
by Cece
NZer1 wrote:Cece are you meaning to say your interested to know what the good Dr has been up to, and even more interested to hear what his mind is finding?
I know I am!
Yes, exactly. We are spoiled here with edge-of-the-seat, up-to-the-minute updates, and I have come to trust Dr. Sclafani's insights as being of high value. He shared the idea of taking post-ballooning CSA measurements very soon after having the idea, and I am curious if he has begun doing so and if he has found anything of interest.

Re: DrSclafani answers some questions
Posted: Sat Jun 30, 2012 4:01 pm
by drsclafani
Cece wrote:NZer1 wrote:Cece are you meaning to say your interested to know what the good Dr has been up to, and even more interested to hear what his mind is finding?
I know I am!
Yes, exactly. We are spoiled here with edge-of-the-seat, up-to-the-minute updates, and I have come to trust Dr. Sclafani's insights as being of high value. He shared the idea of taking post-ballooning CSA measurements very soon after having the idea, and I am curious if he has begun doing so and if he has found anything of interest.
i will resurface asoon to show you an interesting case

, promise
Re: DrSclafani answers some questions
Posted: Sun Jul 01, 2012 6:24 pm
by drsclafani
drsclafani wrote:Cece wrote:NZer1 wrote:Cece are you meaning to say your interested to know what the good Dr has been up to, and even more interested to hear what his mind is finding?
I know I am!
Yes, exactly. We are spoiled here with edge-of-the-seat, up-to-the-minute updates, and I have come to trust Dr. Sclafani's insights as being of high value. He shared the idea of taking post-ballooning CSA measurements very soon after having the idea, and I am curious if he has begun doing so and if he has found anything of interest.
i will resurface asoon to show you an interesting case
, promise
ok, here you go.
A case of very early restenosis
On July 6, 2010 a 51 year old Canadian woman with RRMS was treated in Bulgaria by 10 mm high pressure balloon angioplasty for bilateral internal jugular stenoses and by 7 mm high pressure balloon angioplasty for azygous stenosis. She had remarkable improvements in motor, cognitive, and urinary functions. Balance improved. Fatigue was reduced. EDSS fell from 3.5 to 1.5.
This symptom improvement began to dissipate within a few months. By six months after the procedure, all benefits had disappeared except for fatigue and urinary urgency which no longer caused her discomfort.
In May 2012 she was re-treated by me because of weakness, and numbness in both lower extremities , and a lack of balance.
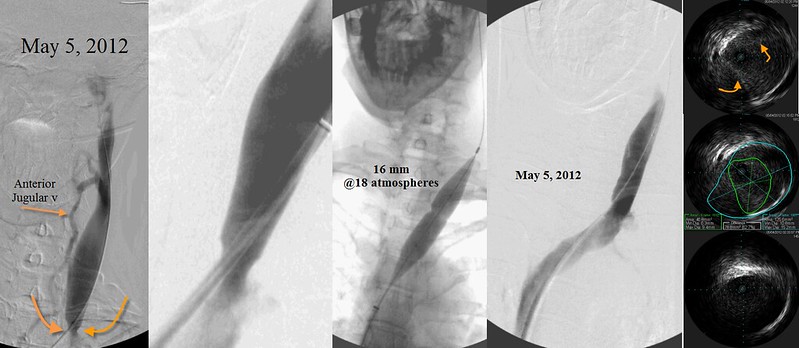
A 60% stenosis of the right internal jugular vein with intracranial reflux appeared to be the result of a septum (orange arrow) that was detected by IVUS. This was treated by larger balloon (16mm) high pressure (18 atmospheres)balloon angioplasty.
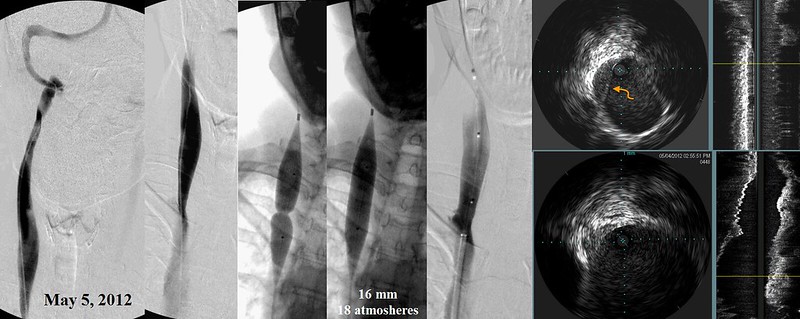
A 85% stenosis of the left internal jugular vein, shown by IVUS to be secondary to immobile valve leaflets, was treated by 16mm high pressure (13 atmosphere) balloon angioplasty.
Not shown, an azygous immobile valve was deteced in the anterior azygous arch and this was treated by a 10 mm balloon angioplasty inflated to 10 atmospheres. A "Nutcracker" syndrome of the left renal vein was also discovered and treated by self expanding stents.
Surprisingly she did not obtain any benefit from this treatment. Indeed she actually felt worse. Her balance deteriorated greatly.
She was observed for eight weeks but no improvements were detected. during that time. I decided to bring her back for a second look.
By that time re-stenosis had already occurred. The venograms lookef essentially the same as before the angioplasties in May. Angioplasties of both internal jugular veins was repeated.


Firstly, I am surprised that relief was achieved with such small balloons in Bulgaria. The vessel seems to look larger than that based upon IVUS. The 16 mm balloons I used certainly were not excessive.
Some say that if there is no response to angioplasty, then treatment of CCSVI is fruitless. . We will know in a couple of months whether that is correct. AT least now we know that failure to improve may result in early re-stenosis within days. or weeks.
I hope that some dialogue can be generated. It took longer to prepare this vignette than to perform the venography.
Re: DrSclafani answers some questions
Posted: Mon Jul 02, 2012 1:39 am
by Robnl
doc,
can it be that the 10mm balloon resulted in 'just enough' flow to get things going?
and maybe the 16mm balloons resulted in too much flow?
Just a thought....
Re: DrSclafani answers some questions
Posted: Mon Jul 02, 2012 5:45 am
by Cece
drsclafani wrote:Surprisingly she did not obtain any benefit from this treatment. Indeed she actually felt worse. Her balance deteriorated greatly.
Here at TiMS and over at the facebook page, we were talking about reperfusion injury recently. It happens in stroke when blood flow returns. Do you think reperfusion injury could be a factor when a patient worsens after successful venoplasty? Is reperfusion injury ever seen when superior vena cava syndrome or carotid artery stenosis is treated?
Firstly, I am surprised that relief was achieved with such small balloons in Bulgaria. The vessel seems to look larger than that based upon IVUS. The 16 mm balloons I used certainly were not excessive.
The 10 mm balloons used in Bulgaria were high pressure balloons. Dr. Zamboni's original patients were treated with 10 mm balloons, but I do not believe those were high pressure. Your original patients in 2009 and early 2010 were treated with 10 mm balloons, following Dr. Zamboni's lead, and I am assuming those were not high pressure balloons. Maybe the high pressure was enough to disrupt the valve leaflets on the one side, even thought it was not enough to stretch the valve annulus itself? And on the other side was a septum. It could be that septums are more easily pushed to the side by venoplasty (thus the response to the 10 mm balloons?) but more likely to return to mid-vein in the weeks or months after venoplasty.
You cannot tell by the venogram that this was a septum? That knowledge was only obtained via IVUS? If septums and valves respond differently to venoplasty, then the ability to differentiate between the two is yet another feather in IVUS's cap.
I hope that some dialogue can be generated. It took longer to prepare this vignette than to perform the venography.
appreciated
Re: DrSclafani answers some questions
Posted: Mon Jul 02, 2012 11:23 am
by drsclafani
Robnl wrote:doc,
can it be that the 10mm balloon resulted in 'just enough' flow to get things going?
and maybe the 16mm balloons resulted in too much flow?
Just a thought....
That is an interesting thought. But i do not think that would explain it nor do i think that too much v enous flow in the jugular vein would be a problem.
Normally veins carry as much flow as is possible. Too much flow is post capillary and that would protect tissue flow and perfusion.
Re: DrSclafani answers some questions
Posted: Mon Jul 02, 2012 1:36 pm
by NZer1
Interesting case.
I have always wondered about the flow changes in areas of the brain from improving flow that is commonly used when one is lying down.
The white and grey matter lesions within the brain are still not interrelated with flow issues found by IVUS for example.
In my example I have 16mm stable hyperintensity at the dorsal aspect at C2 of the cord and 2-3mm focal eliptical area anteriorly in the left centrum semiovale and a more confluent area of white matter hyperinstensity adjacent to the lateral aspect of the atrium of the left lateral ventricle.
*My question has always been what will measure the flow to these regions before PTA and what will the flow change to during PTA and again some months later?
*What has caused the MRI evidence of lesions or hyperintensities to be in regular placings of the Brain in each disease, e.g MS? Then find what the direct cause of the flow issue for the individual flow paths that link to the white and grey matter lesions. At this time these is many, many flow issues and no way to back track the individual findings to connect the flow and lesion effect.
This example Dr. S has given us is helping us see what work is ahead! ;)
I believe changing the flow pattern within the brain is going to create the same effects as flow restrictions in strokes 'in some cases' and that it will be as rapid as the Stroke onset. The flow around the brain is a balancing act because of the chambers and passageways.
The studies required are going to be far more in-depth than what has been historically happening and more accurate symptom gauging is required.
Most of the assessments of symptoms done on PwMS to date have been to find purchasers for drug products rather than understand the conditions such as MS.
Most Neurologists struggle to find clinical symptoms in PwMS because their clinical tests do not define or relate to the symptoms of MS or now CCSVI. BIG changes need to happen!
Food for thought,
Nigel
Re: DrSclafani answers some questions
Posted: Mon Jul 02, 2012 3:55 pm
by tiltawhirl
NZer1 wrote:Interesting case.
I have always wondered about the flow changes in areas of the brain from improving flow that is commonly used when one is lying down.
The white and grey matter lesions within the brain are still not interrelated with flow issues found by IVUS for example.
In my example I have 16mm stable hyperintensity at the dorsal aspect at C2 of the cord and 2-3mm focal eliptical area anteriorly in the left centrum semiovale and a more confluent area of white matter hyperinstensity adjacent to the lateral aspect of the atrium of the left lateral ventricle.
*My question has always been what will measure the flow to these regions before PTA and what will the flow change to during PTA and again some months later?
*What has caused the MRI evidence of lesions or hyperintensities to be in regular placings of the Brain in each disease, e.g MS? Then find what the direct cause of the flow issue for the individual flow paths that link to the white and grey matter lesions. At this time these is many, many flow issues and no way to back track the individual findings to connect the flow and lesion effect.
This example Dr. S has given us is helping us see what work is ahead! ;)
I believe changing the flow pattern within the brain is going to create the same effects as flow restrictions in strokes 'in some cases' and that it will be as rapid as the Stroke onset. The flow around the brain is a balancing act because of the chambers and passageways.
The studies required are going to be far more in-depth than what has been historically happening and more accurate symptom gauging is required.
Most of the assessments of symptoms done on PwMS to date have been to find purchasers for drug products rather than understand the conditions such as MS.
Most Neurologists struggle to find clinical symptoms in PwMS because their clinical tests do not define or relate to the symptoms of MS or now CCSVI. BIG changes need to happen!
Food for thought,
Nigel
That is one awesome post chocked full of the good stuff, right there. It's posts like these that keep me reading here. Thank you.
tilt
Re: DrSclafani answers some questions
Posted: Tue Jul 03, 2012 9:22 am
by drsclafani
drsclafani wrote:
A case of very early restenosis
On July 6, 2010 a 51 year old Canadian woman with RRMS was treated in Bulgaria by 10 mm high pressure balloon angioplasty for bilateral internal jugular stenoses and by 7 mm high pressure balloon angioplasty for azygous stenosis. She had remarkable improvements in motor, cognitive, and urinary functions. Balance improved. Fatigue was reduced. EDSS fell from 3.5 to 1.5.
This symptom improvement began to dissipate within a few months. By six months after the procedure, all benefits had disappeared except for fatigue and urinary urgency which no longer caused her discomfort.
In May 2012 she was re-treated by me because of weakness, and numbness in both lower extremities , and a lack of balance.
A 60% stenosis of the right internal jugular vein with intracranial reflux appeared to be the result of a septum (orange arrow) that was detected by IVUS. This was treated by larger balloon (16mm) high pressure (18 atmospheres)balloon angioplasty.
A 85% stenosis of the left internal jugular vein, shown by IVUS to be secondary to immobile valve leaflets, was treated by 16mm high pressure (13 atmosphere) balloon angioplasty.
Not shown, an azygous immobile valve was deteced in the anterior azygous arch and this was treated by a 10 mm balloon angioplasty inflated to 10 atmospheres. A "Nutcracker" syndrome of the left renal vein was also discovered and treated by self expanding stents.
Surprisingly she did not obtain any benefit from this treatment. Indeed she actually felt worse. Her balance deteriorated greatly.
She was observed for eight weeks but no improvements were detected. during that time. I decided to bring her back for a second look.
By that time re-stenosis had already occurred. The venograms lookef essentially the same as before the angioplasties in May. Angioplasties of both internal jugular veins was repeated.
Firstly, I am surprised that relief was achieved with such small balloons in Bulgaria. The vessel seems to look larger than that based upon IVUS. The 16 mm balloons I used certainly were not excessive.
Some say that if there is no response to angioplasty, then treatment of CCSVI is fruitless. . We will know in a couple of months whether that is correct. AT least now we know that failure to improve may result in early re-stenosis within days. or weeks.
I brought this case up because i think that judging the presence of CCSVI symptoms is often determined by the effects of treatment. There are some treating physicians who are of the opinion that failure to respond, means that the symptoms are not caused by CCSVI. that may be true in many patients, however, i think that this case shows that even aggressive dilatation may not providerelief from valvular or septal obstgructions. We can all understand failure of angioplasty against septal obstructions: the suptum is pushed back against the wall, rather than displaced from the wall and I am certainly challenged by septal obstructions. Very aggressive dilatation may tear the point of attachment of the septum to the wall and provide some relief but the margin for error may be slim. It is certainly not a first line attempted treatment.
But why would valves restenose so quickly if we tear the connection to the valve? I am confident that these valves were opened: IVUS did not show any residual stenosis, nor did venography. Perhaps these valves are so rigid that they will return to the closed position quickly and re-obstruct.To properly study such conditions, I would need funding. repeat venography at short intervals may help gain understand about this type of restenosis. Of course a willing patient. Perhaps surgical removal and pathological evaluation of such valves may provide answers.
But the main point that I am illustrating is that failure to obtain relief after angioplasty does not necessarily mean that "CCSVI treatment is not for you"
Re: DrSclafani answers some questions
Posted: Tue Jul 03, 2012 10:29 am
by Cece
Why did these veins restenose, and will they do so again. Did the treatment in May soften them up for the treatment in July to be successful (not yet known). Where is the funding for the needed research. How do the valves of a patient who experiences this type of restenosis differ from the valves of the patients that don't: are they more rigid.
Much to think about.
Re: DrSclafani answers some questions
Posted: Tue Jul 03, 2012 3:41 pm
by NZer1
Sounds to me like Pathology studies to show what does physically happen with PTA will be needed to take the guess work out of the equation.
If I understand correctly there isn't a way to measure the flows before, during and after PTA, and there is no way of knowing what is popping or tearing under pressure.
I am guessing that until it is understood what re-stenosis looks like we are in the dark.
** Pathology studies would have happened in the past to evaluate Angio in other areas of the Body for other reasons, is it something that crosses over to be accurate when working on Juggs and Azy?
I have always believed that the MS disease is too loose a term and that there are many, many subtypes of the disease and that the Progressive disease is the truest form. Studies on the Vascular involvement on this form in my humble opinion are where the greatest knowledge gain will be. If Pathology studies are used with the focus on the restrictions and pathways back to white and grey matter lesions that will be the inroad to knowledge. The methods of changing the flow issues will again be based on Pathology insights.
The work of the Pioneers such as Dr Schelling will be a good starting point for researchers.
At this time the PTA discoveries may have to go back a step or two and collect data that will be of use to all. A new method of assessing Patients, assessing the condition and management of the deficits is still a work in progress and I hope that fine tuning is evolving the insights.
The Think Tanks need to be happening often and communication open, and willing.
These cases Dr. S is bringing to attention are the ones that will define the future, I again say that Autopsy Research is going to be the fastest and cheapest way to learn what is happening with the methods used to date and the visual understanding of the details in this picture of Life.
Nigel
Re: DrSclafani answers some questions
Posted: Tue Jul 03, 2012 6:04 pm
by mo_en
Hi Dr S. An informative presentation as always.
Why did the veins stayed open for more time after the first procedure in Bulgaria even though the balloons were smaller?
Is there a chance that restenoses were as quick as after your first procedure, but the patient failed to feel them? Or was there something different in the veins themselves when you accessed them in the first place?
Was the septum in the RIJV the result of stuck-together valve leaflets, or some other tissue?
Re: DrSclafani answers some questions
Posted: Tue Jul 03, 2012 6:27 pm
by drsclafani
mo_en wrote:Hi Dr S. An informative presentation as always.
Why did the veins stay open for more time after the first procedure in Bulgaria even though the balloons were smaller?
Is there a chance that restenoses were as quick as after your first procedure, but the patient failed to feel them? Or was there something different in the veins themselves when you accessed them in the first place?
Was the septum in the RIJV the result of stuck-together valve leaflets, or some other tissue?
This is a great question.. I wish I understood why this scenario occurs. Perhaps the improvements from ground zero are so dramatic that they remain so . Could placebo have some impact here? Perhaps improvement in any of the veins leads to an clinical benefit. However perhaps the major effect was the azygous vein. Perhaps restenosis occured in one vein early and as the other vein restenosed clinical symptoms worsened. But why was there no improvement after my angiopplasty? I cannot figure it out The angioplasty was larger and more forceful, yet restenosis occured early. I am so surprised. But i do not yet know what was different in the technique of Dr Petrov compared to my technique. I await some further discussion with Ivo.
Re: DrSclafani answers some questions
Posted: Tue Jul 03, 2012 6:59 pm
by NZer1
Dr. S does having Ultrasound testing give any sort of flow indications in cases like the one above?
It seems it could be to do with the flow improvement by making the valves slightly more open and in still in one piece as opposed to being fully against the wall and then returning/healing to original configuration and symptoms returned prior to seeing you?
Yet the end result was a situation of the valves partial function or total dyfunction destroyed and the residual remains attempting to reattach/heal and recreating a stenosis?
Is there reflux more pronounced and regular now?
The flow speed and volume in each treatment before and after might be of interest?
It would be interesting to be able to identify what the improvement is from the first treatment, it almost sounds like the recovery in some Stroke Treatments?
Is there a problem remaining with CSF flow that hasn't returned to normal or first treatment quality. The CSF flow and symptoms are very similar to CCSVI and MS symptoms?
Problems such as Chiari Malformation issues which are often related to the slowing of CSF because of restricted flow in the region of the Brain Stem (have or share symptoms with MS and CCSVI)?
Changing the vascular flow also changes the CSF and the Arterial flow and all three are interlinked and dependent on each other, change one and you change them all?
Adjustments to the Atlas/C1 are giving in some cases the same benefit as PTA and the flows improvements have been measured, (before and after the adjustment). Results are published by the way. This change in symptoms was attributed to CSF flow changes measured by MR, they occurred as quickly as on table improvements with some PTA? Co-incidence or part of the puzzle?
Having enough information detail with the PTA treatments so that observations can be made and understood with any change in symptoms, BUT which detail, there's a missing piece, what is it, HELP?
Regards,
Nigel