Page 466 of 557
Re: DrSclafani answers some questions
Posted: Wed Jul 11, 2012 9:46 pm
by NZer1
Now that I am getting closer to having some form of treatment my mind has re-engaged with the unknowns in this picture.
** Is there any difference in outcome for people who have active lesions (Gadolinium Injection) on MRI at the time of PTA?
** I have not had active lesions on MRI over a 5 year period yet the lesions appeared in a 6 month space between MRI's and one on my cord was not seen two months ago. Is there a difference in outcomes if a person has stable MRI results at the time of PTA?
** Is a person with RRMS having a difference in the symptom outcome due to the timing of relapses and the PTA Treatment?
** Does the re-stenosis effect after PTA happen across at disease forms, RRMS, SPMS, PPMS and Benign?
** Has there been any symptom outcome that has co-in-sided with an accident, physical stress or any other high pressure cause on the vascular system after PTA?
Regards,
Nigel
# Just saw your comment as I was posting this Cece,
I don't have the access to regular treatment and I don't have the finance for multiple treatments. My disease is not confirmed as MS after 6+ years and I am a slow progressive in what ever is happening (life story, lol). My symptoms started after excessive physical stress on my upper spine and at this stage there is no guarantee of length of benefit from PTA. So I am one to keep a level head and evaluate the options as I see them. If I have IVUS inspection/assessment and down the track there is another option to PTA I still have untouched vein contents and a map of them to look at options at some time! And also Sal will want to retire one day, when will that be, I will feel at a great loss at that time.
Nigel
Re: DrSclafani answers some questions
Posted: Wed Jul 11, 2012 11:43 pm
by NZer1
Abstract positive thought,
If all IR's around the Globe said they will stop doing PTA's on "X day" because the Public is funding what should be funded by "Financial Medical Systems" then the pressure would go onto the appropriate people for investigations.
Imagine that Unity.
It would also define who is in this Industry and for what reasons. This whole situation of feeling in the dark for complex answers could change very rapidly with the right approach!
Lets set a date!
Nigel
Re: DrSclafani answers some questions
Posted: Thu Jul 12, 2012 6:54 am
by 1eye
NZer1 wrote:
** Is there any difference in outcome for people who have active lesions (Gadolinium Injection) on MRI at the time of PTA?
** I have not had active lesions on MRI over a 5 year period yet the lesions appeared in a 6 month space between MRI's and one on my cord was not seen two months ago. Is there a difference in outcomes if a person has stable MRI results at the time of PTA?
vascular system after PTA?
...
And also Sal will want to retire one day, when will that be, I will feel at a great loss at that time.
Nigel
Are you thinking there are Heizenberg effecta that cause as many problems as they solve, due to Gadolinium use or PTA?
And about retirement: perish the thought!! He does want to retire eventually. My father in law drives a truck, puts up and takes down tents and display cases, is on his feet all day, and carries heavy boxes in his "job" twice a week, at age 82. (He also smokes, so no recommendations here.) I would not trust my father-in-law with an IVUS, though. I will feel a loss too, but he has already done so much, that I am grateful anyway.
Re: DrSclafani answers some questions
Posted: Thu Jul 12, 2012 12:25 pm
by NZer1
Note posted by Dr Flanagan on his CCSVI and CCVBP;
"I had a lengthy online meeting with Dr. Rosa today in which he reviewed many interesting cases with me including Chiari malformations, MS and Parkinson's. The imaging and findings are incredible. All of the cases are associated with Chiari 1 type malformation (cerebellar tonsillar ectopia) and maldirected CSF and blood flow. One case showed the tonsils of the cerebellum bouncing back and forth in the foramen magnum due to maldirected flow. Another case showed the cord getting displaced back and forth inside the spinal canal with each cardiac cycle. Several showed turbulance and backjets pounding on the brain and brainstem and compressing them. Several cases have upper cervical lesions where the maldirected CSF flow impacts the brainstem and cord. In some cases the maldirected CSF flow even caused erosion of the bones of the cranial vault. A couple of cases had structural design flaws in the clivus and base of the skull. In one case the clivus is very steep, which as I predicted, makes the brainstem susceptible to Chiari type malformations. That's the short version. Blood vessels are also affected. But that's another story."
Time for people to rearrange their understandings of what "may be" happening into what is imaged by upright MRI!
Regards, Nigel
Re: DrSclafani answers some questions
Posted: Sat Jul 14, 2012 9:12 pm
by drsclafani
drsclafani wrote:
A case of very early restenosis
On July 6, 2010 a 51 year old Canadian woman with RRMS was treated in Bulgaria by 10 mm high pressure balloon angioplasty for bilateral internal jugular stenoses and by 7 mm high pressure balloon angioplasty for azygous stenosis. She had remarkable improvements in motor, cognitive, and urinary functions. Balance improved. Fatigue was reduced. EDSS fell from 3.5 to 1.5.
This symptom improvement began to dissipate within a few months. By six months after the procedure, all benefits had disappeared except for fatigue and urinary urgency which no longer caused her discomfort.
In May 2012 she was re-treated by me because of weakness, and numbness in both lower extremities , and a lack of balance.
A 60% stenosis of the right internal jugular vein with intracranial reflux appeared to be the result of a septum (orange arrow) that was detected by IVUS. This was treated by larger balloon (16mm) high pressure (18 atmospheres)balloon angioplasty.
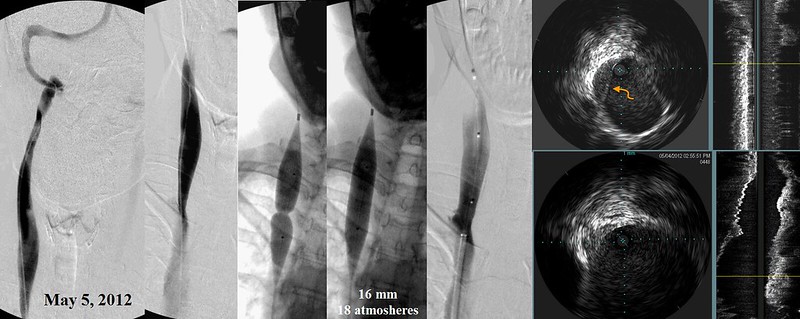
A 85% stenosis of the left internal jugular vein, shown by IVUS to be secondary to immobile valve leaflets, was treated by 16mm high pressure (13 atmosphere) balloon angioplasty.
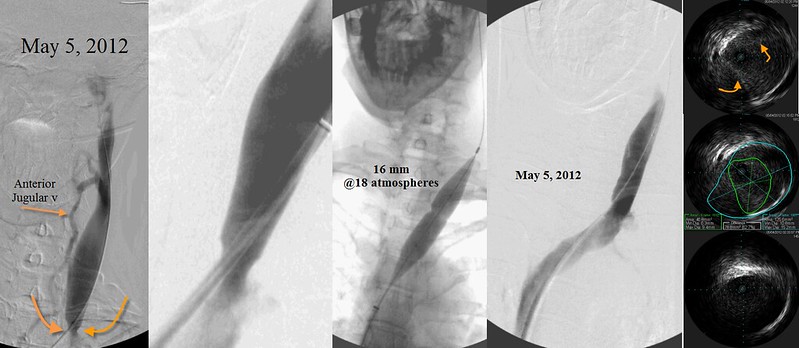
Not shown, an azygous immobile valve was deteced in the anterior azygous arch and this was treated by a 10 mm balloon angioplasty inflated to 10 atmospheres. A "Nutcracker" syndrome of the left renal vein was also discovered and treated by self expanding stents.
Surprisingly she did not obtain any benefit from this treatment. Indeed she actually felt worse. Her balance deteriorated greatly.
She was observed for eight weeks but no improvements were detected. during that time. I decided to bring her back for a second look.
By that time re-stenosis had already occurred. The venograms lookef essentially the same as before the angioplasties in May. Angioplasties of both internal jugular veins was repeated.


Firstly, I am surprised that relief was achieved with such small balloons in Bulgaria. The vessel seems to look larger than that based upon IVUS. The 16 mm balloons I used certainly were not excessive.
Some say that if there is no response to angioplasty, then treatment of CCSVI is fruitless. . We will know in a couple of months whether that is correct. AT least now we know that failure to improve may result in early re-stenosis within days. or weeks.
I hope that some dialogue can be generated. It took longer to prepare this vignette than to perform the venography.
This is the followup on the patient presented as an early restenosis
here is an update of my situation two weeks after the june 29th intervention :
-contrary to the may 4th intervention where i had not seen any improvement of my condition, i felt much better 24 hrs after the june 29th intervention , and still continue to feel much better after two weeks : better equilibrium , better legs strenght , better ability to walk ,brain fog significant diminution , sensitivity under my feet , fatigue sensation almost disappeard......
conclusion: A HUDGE IMPROVEMENT OF MY CONDITION 24 HRS AFTER THE INTERVENTION wich is STILL THERE AFTER TWO WEEKS.
THANKS TO YOU , THANKS TO YOU ....
It is so unfortunate that patient insurance is not possible. It is just not possible to repeat procedures without some additional revenue. I am sure that there are many patients with early restenosis that are thought of as failures.
Re: DrSclafani answers some questions
Posted: Sat Jul 14, 2012 9:59 pm
by NZer1
This is fantastic news!
** Dr S have you ever had anyone that has not improved after a second IVUS inspection? This question comes to mind because of the Dr Rosa and Dr Flanagan insights that I have been posting. This 'could' be an amazing opportunity to have such a person do the study.
Regards Nigel
Re: DrSclafani answers some questions
Posted: Sun Jul 15, 2012 3:21 am
by CureOrBust
drsclafani wrote:I am sure that there are many patients with early restenosis that are thought of as failures.
Did she show up clearly as having flow issues from the restenosis, using U.S.?
Re: DrSclafani answers some questions
Posted: Sun Jul 15, 2012 11:00 am
by drsclafani
NZer1 wrote:This is fantastic news!
** Dr S have you ever had anyone that has not improved after a second IVUS inspection? This question comes to mind because of the Dr Rosa and Dr Flanagan insights that I have been posting. This 'could' be an amazing opportunity to have such a person do the study.
Regards Nigel
Nigel
yes, i have had patients who did not improve after a second procedure.
But this is a special situation. A patient who had fleeting improvements after the first procedure, then lost all benefit. The second procedure was done very early, earlier than anyone i have ever treated (except for aggressive treatment of early thrombosis). I have never had proof of such early restenosis. The second early treatment re-opened the stuck valves.
Now we wait to see whether restenosis occurs again. if it does, we will consider stents.
This scenario of very short term improvements has occurred in the past but because of costs, early second treatments was not realistic . We got lucky in this situation and discovered something. I am not trying to figure out how to price early second procedures at discounts.
DrS
Re: DrSclafani answers some questions
Posted: Sun Jul 15, 2012 11:05 am
by drsclafani
CureOrBust wrote:drsclafani wrote:I am sure that there are many patients with early restenosis that are thought of as failures.
Did she show up clearly as having flow issues from the restenosis, using U.S.?
CureOrBust,
I would not need to perform a CCSVI Zamboni protocol ultrasound in this situation. The diagnosis of CCSVI was already made. She did have an ultrasound at one month in Canada, which I routinely have my patients get locally to look for thrombosis. However no thrombosis was noted.
When she returned to NYC, i didnt resort to another ultrasound, but rather when directly back to venography, detected the stenosis and re-treated it with similar or slightly larger balloons (I dont remember off hand).
I didnt know whether this would help her, but th ankfully it has. Now we wait to see if the valves stay open.
DrS
Re: DrSclafani answers some questions
Posted: Sun Jul 15, 2012 11:41 am
by 1eye
It's still early to declare a victory, but do you think ballooning twice over this short a time could turn out to make the thing last longer? I realize you would only do it for restenosis.
Re: DrSclafani answers some questions
Posted: Sun Jul 15, 2012 12:07 pm
by drsclafani
1eye wrote:It's still early to declare a victory, but do you think ballooning twice over this short a time could turn out to make the thing last longer? I realize you would only do it for restenosis.
I quote wilhelm roentgen when asked by reporters what he thought when he first saw the glow coming off the cyanobarium platinum plate when he aimed the xray apparatus on it
I did not think, I investigated
Re: DrSclafani answers some questions
Posted: Sun Jul 15, 2012 11:50 pm
by NZer1
Hi Dr,
putting your quote into different terms for us lay people, does this mean that the use of IVUS maybe a way of understanding the different problems you are finding, and giving an indication that some will benefit from a second treatment in a new time/healing process understanding.
Shorter 'Time factor' for a second PTA being of benefit because of the advancing healing processes that are hindering the objective, flow.
Regards
Nigel
Re: DrSclafani answers some questions
Posted: Mon Jul 16, 2012 11:04 am
by dlb
Dr. Sclafani,
Regarding your last case study and other patients whose veins don't remain patent..... Is something like Ehlers Danlos at play, where collagen is not typical? Is that a possibility for veins not holding up after venoplasty? Just thoughts I have.... We are all so different!
Re: DrSclafani answers some questions
Posted: Tue Jul 17, 2012 10:18 am
by mo_en
Dr S, do you find LIJVs getting restenosed/thrombosed more frequently than RIJVs?
Re: DrSclafani answers some questions
Posted: Wed Jul 18, 2012 2:22 pm
by drsclafani
NZer1 wrote:
I believe changing the flow pattern within the brain is going to create the same effects as flow restrictions in strokes 'in some cases' and that it will be as rapid as the Stroke onset. The flow around the brain is a balancing act because of the chambers and passageways.
The studies required are going to be far more in-depth than what has been historically happening and more accurate symptom gauging is required.
Most of the assessments of symptoms done on PwMS to date have been to find purchasers for drug products rather than understand the conditions such as MS.
Most Neurologists struggle to find clinical symptoms in PwMS because their clinical tests do not define or relate to the symptoms of MS or now CCSVI. BIG changes need to happen!
Food for thought,
Nigel
Nigel, it is always difficult to respond to your hypotheses because they are so complex, filled with wisdom and also filled with concepts that i dont agree with or that are hypotheses that I cannot refute.