aliki wrote:thank you very much for your answers . I restarted taking coumadin and I feel better . I will try to find a good acupuncture place to have some treatments . My left jugular vein that is clotted creates lots of problems ..
Dr Sclafani could not treat my left jugulae vein because it was clotted and he couldn't do anything . The clot was very hard .
I feel a little better than before but I continue to have ccsvi problems , fatigue, cog fog , dizzyness and the worst thing is that now I cannot see well the colors and my ears have a tinning . These are new, before the procedure I didn't have that even after my last relapse 2 days before the procedure I was seeing good the colors and there was no tinning . Did this happen to anyone else ? I do patience but I really feel awful . I believe that something didn' t go well in my case but I don't know what is this ..
dania wrote:you are not the only one. All my veins that had angioplasty died.They became stringy dried strands. Zero blood flow. It seems the less blood flow the more disabled one becomes.
Sorry Dania, the loss of these jugular veins is very sad.
thrombosis is related to a variety of causes, inadequate flow or stasis, inciting material in the vessel, damage of the venous wall, the degree of coagulability of the patient
thrombosis is a complication of angioplasty. Angioplasty stretches the vascular wall and this results in exposure of the muscle in the venous wall to the circulating blood. the exposed muscle chemically signals the platelet cells to aggregate to each other and to the injured wall and initiates the clotting cascade. thus angioplasty increases risk of thrombosis.
I treat my patients with a thrombin antagonist and platelet inhibition to retard the natural reaction during the healing process. Unfortunately it doesnt always work and thrombus may still occur. It happens in my practice in about 1.5% of my patients.
To try to salvage such situations, treatment of thrombosis must be swift. Untreated thrombus quickly organizes into a dense fibrotic situation that can result in loss of the vein as in dania's experience.
at the completion of my prophylactic regimen, I recommend a sonogram to find thrombosis early.
the following example represents such a case.
this 54 year old man was treated previously by another interventionalist with short term clinical improvements. I retreated the patient.

The upper images show reflux in the occipital emissary veins. There was a stenosis of the inferior jugular bulb shown on IVUS to be caused by an immobile valve (top right). The two lower left images show an inflated balloon with two annular constrictions. While the lower one was eliminated, the upper one did not resolve despite several dilatations up to 22 atmospheres. Nonetheless, the image on the far right seems show a good dilatation and improved flow.
He was treated by pradaxa 150 mg every 12 hours for thirty days, accompanied by a daily 81 mg aspirin. After treatment the neck was sore, but no improvements ensued. Nothing seemed to change clinically except three days before i saw him in followup he had a day of intense fatigue. on the day i saw him his assessment was unchanged from prior to the procedure five weeks ago. An ultrasound was performed as is our routine and he had thrombosis of the right internal jugular vein, manifested on ultrasound by an absence of color flow in the lower third of the vein and by a lack of compressibility of the jugular vein.
He returned to the procedure suite the following morning. The images of that event (yesterday) were as follows
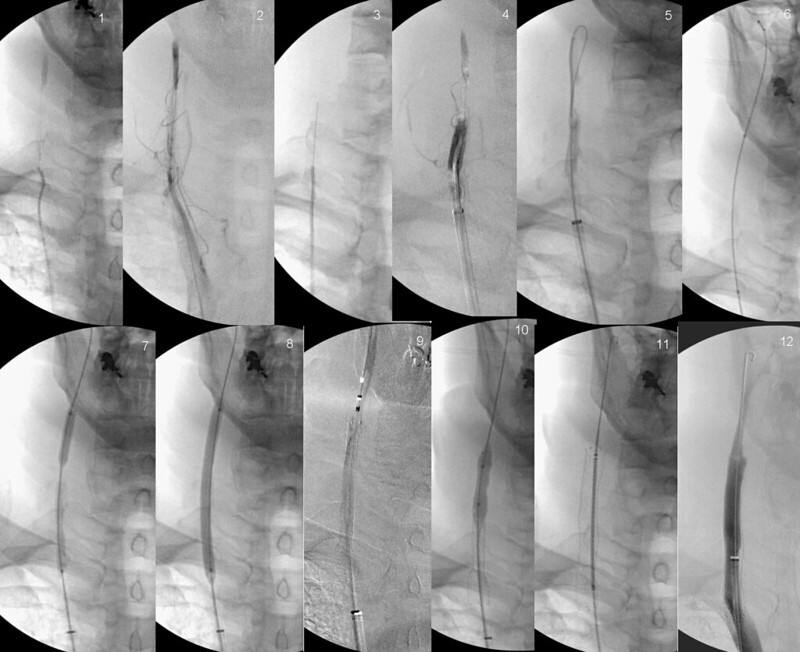
images show the following:
1&2. the tip of the catheter is in the tip of the occluded vein: a fine line of contrast media indicates the existing size of the lower internal jugular vein. some contrast fills the upper IJV, not thrombosed.
3. The stiff end of a fine wire was advanced very carefully up the channel. You see where the tip ended. it was impossible to push it further up the vein, probably because of fibrin plug is preventing that from occurring.
4. The catheter was advanced up that wire and contrast study shows that part of the vein is filled with liquid clot. However the appearance extending up to the patent vessel remains a thin track.
5. using a stiffer wire looped around was pushed through the upper plug into the vein that was patent.
6. Finally a catheter extends across the obstruction and now linking the brachiocephalic vein to the upper jugular vein.
7. A thin balloon catheter was extended up along the wire and inflated. This creates a channel that can accomodate the larger stent catheter.
8. The balloon is finally fully inflated.
9. a stent is deployed. Self expanding nitinol, it opens at body temperature at it is uncovered.
10. A balloon is inflated to open the stent.
11. The stent is completely expanded to 10 mm.
12. Flow has been restored.
Now we must resume anticoagulation as the vein attempts to heal itself.
Any questions.
4.
2.