Cece wrote:drsclafani wrote:cece
i am close to completing a very interesting case study that i will share shortly
DrS
I am interested.

And welcome to the thread, Luke!
Welcome Luke. Cece as promised:\
The patient is a 41 year old woman american of asian background who was diagnosed with relapsing remitting multiple sclerosis at the age of 26, but her symptoms began two years earlier at the age of 24. Her last relapse was in August 2010, which occurred five months after completion of 36 treatments with Tysabri. About five months after that treatment, she developed back weakness and lost movement in both legs. She was treated with steroids at that time and her spine strength improved, but her legs did not regain strength. She states that her symptoms include cognitive, motor, sensory, and autonomic abnormalities.
In Spring 2010 she became the second patient of an early adopter of interventional treatment of ccssvi
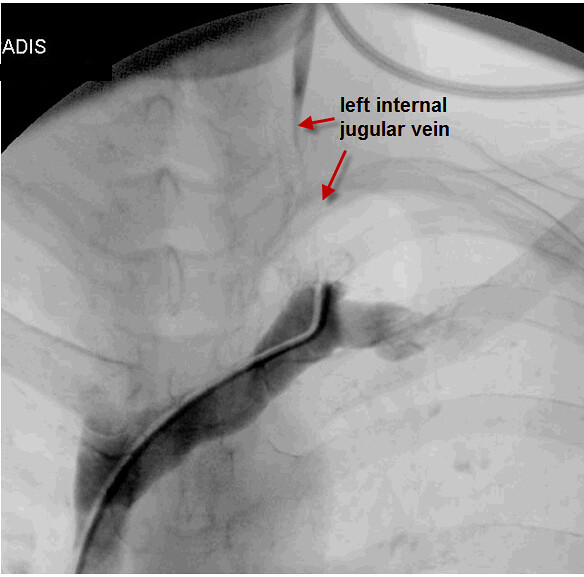
FIRST LEFT INTERNAL JUGULAR VENOGRAM

Left image: catheterization of the left internal jugular vein was difficult and contrast study at its orifice does not show the vessel. The image on the right is the left vertebral vein. Since the study was called normal, it is possible that this injection of the vertebral vein may have been misinterpreted as a normal internal jugular vein.
FIRST RIGHT INTERNAL JUGULAR VENOGRAM

This was interpreted as normal and no intervention was performed.
The left image is an injection below the the right internal jugular valve. The black arrow points to the location of the funnel of the stenosis of the vaalve. The orange arrows show dilatation of the area below the valve caused by pressure elevations as the flow goes through the obstructed valve, very much like the pressure of water in a hose increases when you put your finger over the end of the hose.
the image on the right shows the dilatation of of the vein below the stenosis. the pink arrow points to a large anterior jugular vein that is bridging the obstruction of the jugular valve. This vein should not be visualized so prominently in the absence of an obstruction.
-----------------------------------------------------------
After reviewing her images, subsequently, the interventionalist tried a second procedure in the Fall of 2010. She agreed to a second catheterization.
SECOND RIGHT INTERNAL JUGULAR VENOGRAM

on the repeat venogram the findings mentioned above were recognized and balloon angioplasty. Look how the inflated balloon is about the same size as the vein itself. I would think that this is likely going to be too small a balloon. You can see that the stenosis was still present on the image after angioplasty (on the RIGHT). No further angioplasty was done.
SECOND LEFT INTERNAL JUGULAR VENOGRAM

On this venogram of the left IJV the interventionalist finally gets the catheter across the stenotic valve. Stenosis is now seen. It was treated but there were no images of the venoplasty on the patient's CD.
SECOND AZYGOS VENOGRAM
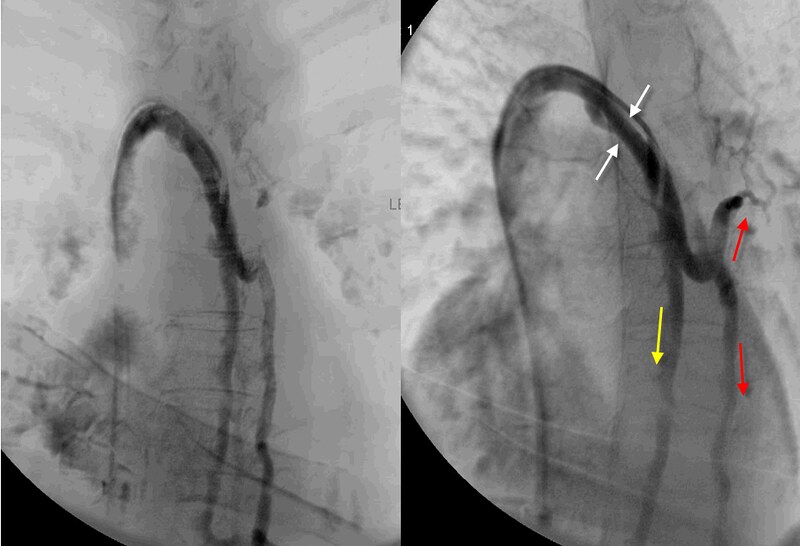
I havent shown the first azygous venogram because it was also not on the patient's CD.
This second azygos venogram shows reflux down the azygos vein (DOWNWARD YELLOW ARROW) and down the hemiazygos vein (DOWNWARD RED ARROW). Also there is enlargement and reflux in the accessory Hemiazygos vein (UPWARD RED ARROW). This could be a hemodynamic manifestation of obstruction or high flow. Perhaps there is a stenosis in the azygos arch. (WHITE ARROWS) An angioplasty was performed in the azygos vein but it was unclear where that angioplasty was performed. No definite site of obstruction was determined so i think that angioplasty of the entire azygos vein was performed.
_____________________________________________
She had symptomatic improvement after this venoplasty. Sleep was better, vision was clearer, cognition and memory were better. The left hand and arm and both legs became stronger, voice improved. These improvementsi lasted about one week. A followup ultrasound done one week after treatment showed that the left jugular vein had thrombosed. All improvements vanished and disability increased about three weeks after treatment. She was anticoagulated.
___________________________________________
In 2011 she underwent a third procedure by different interventionalist.
THIRD LEFT JUGULAR VENOGRAM
the interventionalist was able to engage the orifice of the left internal jugular vein but it appears that he did not attempt recanalization of what he thought was a small vein. I think that this was unfortunate because it turned out to be the last opportunity to attempt restoration of flow through this vein.
THIRD AZYGOS VENOGRAM
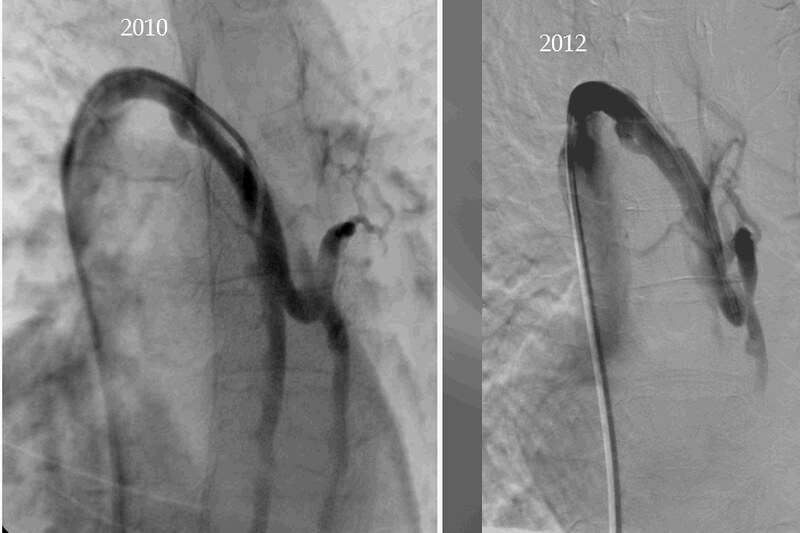
The azygos vein seems occluded at this time. It is shrunken, narrrowed and irregular in 2012 compared to 2010. The ascending portion does not fill like previously. Azygos arch stenosis is still present. Reflux into the accessory hemiazygous vein is still also seen.
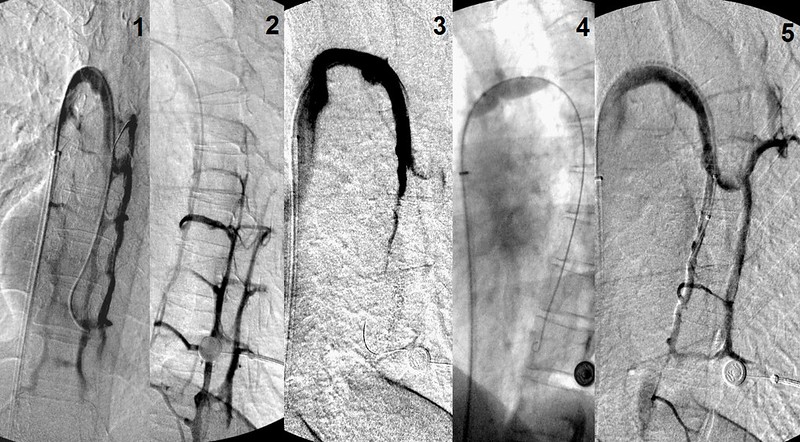
THIRD RIGHT INTERNAL JUGULAR VENOGRAM

This is a composite of the treatments of the right internal jugular vein by both interventionalists. Neither attempt to dilate this valvular stenosis was successful because neither actually showed opening of the valve on their confirmatory venogram after venoplasty. A larger balloon was likely necessary to get this stuck valve open.
The patient did not obtain noticeable improvements after this round of treatment.
_______________________________________
I consulted with this patient in early January. She presented to me with paralysis, ataxia, spasticity, chronic fatigue as her major complaints. Examination was consistent with extensive pyramidal tract as well as cerebellar disease. She underwent an ultrasound of the jugular veins and deep cerebral veins on January 10, 2013, which revealed reflux in the upright and supine positions in the right internal jugular vein and in the deep cerebral veins, as well as episodes of no flow in the right internal jugular vein. B-mode abnormalities including thickened, immobile, elongated valves and other intraluminal echogenic foci were also noted on the right side. The left internal jugular vein was thrombosed and there were large collaterals in the left side of the neck as well as prominent left thyroid veins.
FOURTH RIGHT INTERNAL JUGULAR VEIN VENOGRAPHY

As you can see on the images on the left, valvular stenosis persists. I think you will be interested to see that while two angoplasties have been performed, NO stenosis of the surrounding vein has taken place. I really do not think that stenosis of the dilated segment occurs in this disease as often as in other diseases of veins. Those stenosis are usually the result of surrounding scar tissue which is not generally present in CCSVI. I think that the pathology in CCSVI is NOT similar to other causes of stenosis. Unless gross over expansion of the vein occurs, or perhaps, if prolonged dilatations are performed, stenosis of the surrounding vein is not a common or expected feature of ccsvi treatment.
I used a 14 mm balloon to perform angioplasty and the post angioplasty image looks better but still valvular stenosis remains. IVUS confirmed that the valve remained stiff and fixed. Therefore I used a 16 mm balloon and after this the vein looked wide open both on IVUS and venography.
I tried to access the left internal jugular vein in the neck but this was not possible.
FOURTH AZYGOS VENOGRAPHY
These images show a lot of reflux into the intercostal veins and other collaterals. I decided to leave the naturally recanalzed ascending azygos alone. I did not think I could make it much better and actually risked making things worse. I do not know whether this is a correct decision but better to come back another time than risk making things worse.
FIRST RENAL VENOGRAM
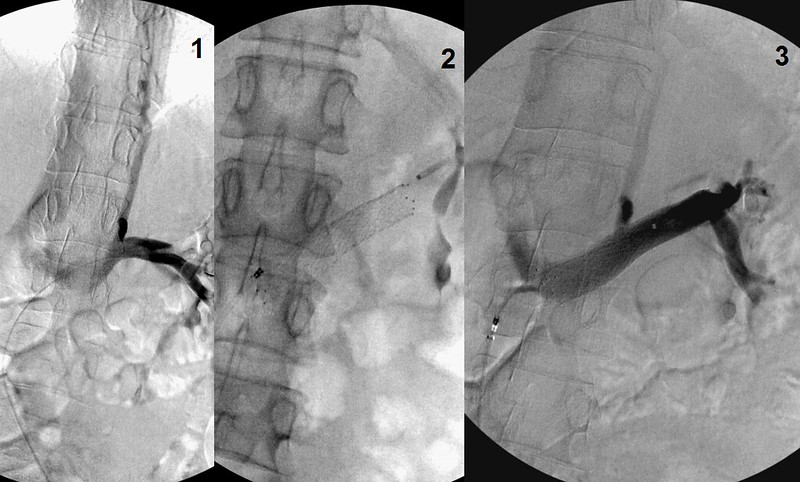
This is a really interesting finding. The left renal vein is lower than it usually enters the inferior vena cava. I thought that it was a posterior nutcracker. This is a less common varant, in which the left renal vein runs behind the abdominal aorta and the compression is between the aorta and the vertebral column. The usual compression is between the aorta and the mesenteric artery. Either way the treatment is the same.
There is reflux into the distal hemiaygous vein through the hemiazygo-renal trunk. Given the disease in the azygous itself, I imagine there is venous congestion of the vertebral plexus of veins and congestion in the spinal cord. A patient with a occlusive disease of both the azygos and the left internal jugular vein cannot adapt to the augmentation of cerebrospinal venous circulation. n the absence of jugular and azygous outflow obstructions, This renal venous obstruction really congests the spine.
it is too early to tell whether this new round of treatments will lead to a successful clinical outcome. the lessons learned are
1. balloon size seems to m atter. It is also apparent that even minor dilstations can be helpful but insufficient dilatation may lead to early loss of improvements
2. occlusion of the vein are challenging. It is difficult to predict which veins weill occlude. Certainly patients wth hpercoagulaable states, very small dural sinuses, poor flow through the upper jugular vein, and large collaterals that may continue to siphon venous blood throubh a collateral are at risk.
3. attempts are recanalization
4. IVUS is really important in discovering sites of valvular stenosis.
5. it does not appear that repeated angioplasties do not necessarily result in stenosis of the vein but rather to restenosis of the valve alone.
Nutcracker is common in patients with MS.