Page 505 of 557
Re: DrSclafani answers some questions
Posted: Sun Jan 27, 2013 10:21 pm
by drsclafani
EJC wrote:drsclafani wrote:EJC wrote:Dr S.
I follow this thread, despite not understand a reasonably large amount if it, I do try.
The fact you're here and spend the time discussing this subject in such detail with your patients and anyone else wanting to ask questions is simply outstanding, like you haven't got enough on your plate already. What I'm trying to find though is an overview of your thoughts. Not particularly just medical detail, but how you feel about where you are with CCSVI and where CCSVI is with MS patients.
Do you feel you understand CCSVI more than ever or as you've delved deeper into the subject are you still raising more questions than answers?
When you see a new patient do you feel a CCSVI procedure stands a good chance of helping them?
My wife had CCSVI treatment in Scotland in Dec 2010 and had very promising results (particularly eyesight improvements) which gradually regressed over the next 9-12 months. In Dec 2011 she had jaw realignment work in London which I'm documenting on this forum, with fantastic results.
Each treatment/procedure had a direct effect on different symptoms.
CCSVI returned warmth to my wifes hands and feet, reduced cog fog and provided an instant and substantial improvement in eyesight. Much of this regressed.
Jaw realignment eradicated debilitating neuralgia in her left arm, hand leg and foot. It also has reduced substantially the amount of fatigue she suffered from a daily "battery" life of awake hours of 6-7 hours to a near normal 12-14 hours. Rather than any sign of these regressing they are continuing to improve as time passes, to a degree that phyio and physical rehabilitation has begun to get her back on her feet and more mobile (EDSS reached 6.5 but now starting to improve).
As a layman I look at these results and see two treatments offering relief of two clear sets of symptoms. These are the questions that run through my mind.
1. Was my wife under treated for CCSVI (quite rightly at the time) as we were in the early stages of the development of the treatment two years ago?
2. Have we actually found two things my wife needed treating for but gone about it in the wrong order?
3. Is there any connection at all between skeletal misalignment/TMJ disorders and CCSVI? Or have we simply discovered my wife has two separate ailments providing symptoms currently known to medicine as MS?
4. Once treatment for My wifes TMJ problem are complete would she benefit from a further CCSVI procedure based on the initial improvements of the first procedure?
I'm not actually sure I even expect an answer, I'm typing this more to share my thoughts rather than look for something definitive. But I would really like to know where you feel you are at the moment with CCSVI, globally. In laymans terms.
TIA.
That is a great question. The answer would be very complex, and require quite a bit of thought. So a pat five line answer won"t do it. Let me sleep on this one for a while. please pose the question at the new year. I think that will be a fitting time to look back. Since i do not sleep very much, i will need that much time to formulate my reply.
Well, it's January. I know you've covered a few of the topics in my questions above but I wondered if you've now managed to sleep on it for a while and come up with a global answer to "Where are with CCSVI right now Dr S?"
still working on this. If you dont mind, i think it will be better to wait until after the ISNVD meeeting in February. There is much new material to be presented.
Re: DrSclafani answers some questions
Posted: Sun Jan 27, 2013 10:28 pm
by drsclafani
helenaz wrote:Hi,
I am writing from Poland, i am here first time. I have a question to Dr Sclafani and everybody else, does exist natural treatment which works similar to ccsvi surgery? maybe some herbs or something else? thanks for answers, Luke
dear luke
firstly welcome
secondly we do not consider the interventions that we perform to be surgery, but rather minimally invasive therapies. I, for one, do not use a scalpel for this procedure. All my patients are awake during the treatment. I do not put my patients to sleep for this procedure. Most of the procedures are performed by interventional radiologists rather than surgeons.
Now, is there a natural treatment that will relieve obstructed valves, and other stenoses. I am afraid that there are not. These are mechanical prolblems. We have some contraversy about which treatments are valuable, and there are medications and over the counter remedies that can enhance venous health, reduce inflammation etc, but adhesions of a valve are not going to be dissolved by any substance I am aware of
Re: DrSclafani answers some questions
Posted: Sun Jan 27, 2013 10:33 pm
by drsclafani
Flashover81 wrote:Hi Dr. S. I am the father of a 16 almost 17 year old son who presented with ataxia and nystagmus at age 14 almost 15. Diagnosed initially with ADEM, had MRI at 6 months looked good leisions starting to go away "leisions were prdominately Periventricular". Second MRI showed a new leision so he was tagged with MS. He has had no other episodes since the first one almost 3 years ago.
He is not on any DMD. We have been trying to eat healthy and taking supplements D3 5000IU a day and Protandim. I can't say if this works or not it can't hurt.
The only thing abnormal my son has is Angiodema. It can swell his lip to twice it's size or swell his eyes shut. When he swells it looks like he was in the worst fight of his life lol. I feel this is caused allergies because we treat it with Claritin. But it just seems maybe in his case there might be a correlation there.
Have you treated or heard of PWMS having Angiodema?
Thanks Jimmy.
Jimmy
sorry for your troubles. It must be a very trying thing to have to deal with MS in someone so young. I am happy that your son is relapse free.
I think the angioedema is likely to be allergic in nature, although patients with MS may have imbalance of sympathetic and parasympathetic companents of the autonomic nervous system. and edema is not uncommon, bot mostly in the lower extremities.
What does your allergist say?
DrS
Re: DrSclafani answers some questions
Posted: Mon Jan 28, 2013 12:12 am
by NZer1
Dr S when you discuss the findings from examples like the one you have shown above with the original IR's what sort of responses do you get?
I imagine in this case the IR's would have had more experiences over time and they themselves would have opinions of their prior work.
Do you make contact with the IR's so they will learn and grow from the experiences or is it only those who look on here (TiMS) or hear you speak at conferences or other media?
The IVUS benefit in many of these examples would sell the advantages of the technology?

Nigel
Re: DrSclafani answers some questions
Posted: Mon Jan 28, 2013 1:52 am
by helenaz
Dr. Sclafani,
Thanks for response, I understood. Could you tell more about "medications and over the counter remedies that can enhance venous health, reduce inflammation etc" ? Could you give any examples of this kind medications?
Thanks a lot, Luke
Re: DrSclafani answers some questions
Posted: Mon Jan 28, 2013 11:11 am
by Cece
drsclafani wrote:it is too early to tell whether this new round of treatments will lead to a successful clinical outcome.
Compared to her hemodynamics prior to any procedures
a ) she had a completely obstructed left jugular and now has a completely occluded left jugular so this would seem to be equal in terms of flow
b ) she has improved flow in the right jugular
c ) she has diminished flow in her azygous vein
d ) she has improved flow in the renal vein which means a considerable amount of flow is no longer being directed to the azygous or lumbar veins
Is her flow better or worse now than it was prior to any procedures? Does opening the right jugular and opening the renal vein compensate for the azygous occlusion?
Disability increased after the second procedure; this would be when the azygous occluded. It seems plausible that the combination of nutcracker syndrome and azygous occlusion is worse than azygous occlusion alone. Nutcracker has now been treated.
Wouldn't the increased flow from the nutcracker syndrome have been a benefit making it less likely that the azygous would thrombose? Although obviously it occluded.
Re: DrSclafani answers some questions
Posted: Mon Jan 28, 2013 11:29 am
by Cece
drsclafani wrote:the lessons learned are
[...]
4. IVUS is really important in discovering sites of valvular stenosis.
These images where stenoses were present but failed to be diagnosed, such as you showed above, make for very useful learning tools.
I worry about pwMS getting a '2010' treatment in 2013. Depending on the experience of the provider.
Re: DrSclafani answers some questions
Posted: Mon Jan 28, 2013 11:36 am
by Cece
This was a complex case study even to read. I have to think it took longer than usual to prepare.
A followup ultrasound done one week after treatment showed that the left jugular vein had thrombosed. All improvements vanished and disability increased about three weeks after treatment. She was anticoagulated.
I misinterpreted this on my first read through, thinking you were saying that the thrombosis occurred despite being anticoagulated. Now I read this as that the response to the left jugular thrombosis was to anticoagulate. Was she not anticoagulated before? If you caught a thrombosis at one week out, would your standard of care be to do a manual endovascular removal of the clot if possible? I was rereading to see if lack of follow-up care contributed to the occlusions but this thrombosis was caught very early.
Re: DrSclafani answers some questions
Posted: Mon Jan 28, 2013 11:40 am
by Cece
drsclafani wrote:SECOND LEFT INTERNAL JUGULAR VENOGRAM

THIRD LEFT JUGULAR VENOGRAM
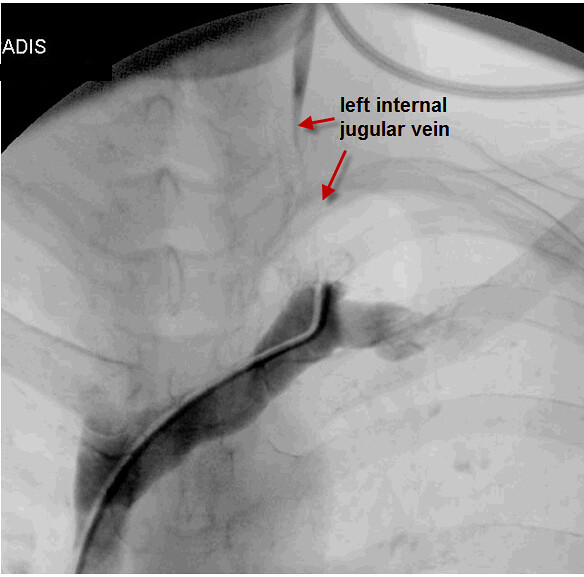
I suggested above that the obstructed left jugular prior to any procedures and the occluded left jugular after procedures would be similar in terms of hemodynamics. Looking at the images, it's obvious that I was wrong and the occluded jugular is much worse.
The azygous, however, naturally recanalized in the ascending portion (if it is a candy cane, this is the stick of the candy cane) so the azygous is not as bad off as I thought on the first read-through. It even looks as if ballooning of the arch of the azygous was done on this most recent procedure.
Re: DrSclafani answers some questions
Posted: Mon Jan 28, 2013 12:06 pm
by NZer1
Cece imagine what would be learned from Dr Zamboni's collar testing!
Before, during and also after tests over time...............
Re: DrSclafani answers some questions
Posted: Mon Jan 28, 2013 12:23 pm
by Cece
NZer1 wrote:Cece imagine what would be learned from Dr Zamboni's collar testing!
Before, during and also after tests over time...............
Collar testing plethysmography would be helpful in this case if it showed that the patient now had normalized results. I don't know if that's possible to have normal results with only one jugular functioning. But there must be a spectrum from normal or near-normal all the way to severely impaired. It's a win if we move towards the normal end of the spectrum even if we don't get all the way there.
Re: DrSclafani answers some questions
Posted: Mon Jan 28, 2013 12:51 pm
by NZer1
Cece I think when we look at one part of a system eg the neck and or chest and don't consider the entire picture eg the sinuses or the VV's then we need to find out what is happening before during and after and also we desperately need to understand what is minimal requirements for Life!
The collar concept must have come about in Zamboni's mind as well. Non-invasive tests to compare what works with what isn't and find the reasons for dysfunction.
We Human's designed computers and realise that it is a symbiotic relationship that keeps a computer functioning yet we don't look at ourselves holistically.
Nigel
Re: DrSclafani answers some questions
Posted: Mon Jan 28, 2013 2:49 pm
by Cece
drsclafani wrote:EJC wrote:Well, it's January. I know you've covered a few of the topics in my questions above but I wondered if you've now managed to sleep on it for a while and come up with a global answer to "Where are with CCSVI right now Dr S?"
still working on this. If you dont mind, i think it will be better to wait until after the ISNVD meeeting in February. There is much new material to be presented.
http://tinyurl.com/amrh2aj
Much new material!
Nigel, here's one: Interpretation of cervical plethysmography data with respect to the diagnosis of CCSVI. Clive B. Beggs (UK)
And this one: Comparison of IVUS to gold standard catheter venography for detection of extra-cranial venous abnormalities indicative of CCSVI: results of the PREMiSe study. Yuval Karmon (USA)
and more!
Re: DrSclafani answers some questions
Posted: Mon Jan 28, 2013 3:39 pm
by NZer1
Thanks Cece,
can you check the url please, I can't get anything!
Ta,
Nigel
Re: DrSclafani answers some questions
Posted: Wed Jan 30, 2013 1:04 pm
by drsclafani
Anonymoose wrote:Hi Dr. Sclafani,
Thank you for reaching out to us greenies.
I've got a question for you.
Can you in any way substantiate or disprove the suspicion that CCSVI angioplasty renders improvement in MS patients by reducing neurovascular contact in the medulla region between veins, the rostral ventrolateral medulla, vagus, glossopharyngeal, and vestibulocochlear nerves?
I guess i have procrastinated long enough on answering anonymoose's question.
i struggle with theoretical issues because sometimes answers are taken out of context or as definitive explanations of things. I am not at all convinced of your explanation. My own sense is that the veins, even obstructed veins, are not under great pressure. Think about the adjacent arteries that are at pressures 15-20 times greater than the veins.
my own sense is that cranial nerve and hypothalamic compression is more likely the culprit here. Increases in cerebrospinal pressure probably related to venous outflow reduction's negative effect on cerebrospinal flud drainage causes some minimal increases in pressure in the CSF and downward movement of the brainstem toward the foramen magnum. I think that the compression of the brain stem at the foramen magnum is subtle but may be significant. I certainly have an easier time accepting nearly instantaneous improvements explained by improved CSF drainage than effects on the Vagus nerve.
Not definitive but my sense of things.
S