This Is MS Multiple Sclerosis Knowledge & Support Community
Welcome to This is MS, the leading forum for Multiple Sclerosis research and support. Join our friendly community of patients, caregivers, and researchers celebrating over 20 years of delivering hope through knowledge. https://www.thisisms.com/forum/
Oh, and for the first two treatments I was not prescribed any blood thinners post op.
Wild Wild West out there.
There would have been heparin used during the procedure but that's for a short time only.
Heparin is used to treat deep vein thrombosis: http://emedicine.medscape.com/article/1 ... #aw2aab6b3
Re: DrSclafani answers some questions
Posted: Wed May 08, 2013 7:03 am
by drsclafani
Cece wrote:
Oh, and for the first two treatments I was not prescribed any blood thinners post op.
Wild Wild West out there.
There would have been heparin used during the procedure but that's for a short time only.
Heparin is used to treat deep vein thrombosis: http://emedicine.medscape.com/article/1 ... #aw2aab6b3
There are preferences among doctors. It is not all wild wild west because not everything is so clearly defined by data. For example, i do not use heparin during the procedure. I really cannot point to good evidence. However, the anecdotal intracranial hemorrhages occurring immediately during or after some procedures reported on the internet may have resulted from procedural anticoagulation. Thus i have avoided giving heparin during procedures. No class 1 evidence, but just a reasoned judgment.
Re: DrSclafani answers some questions
Posted: Wed May 08, 2013 7:05 am
by drsclafani
NZer1 wrote:
CureOrBust wrote:
NZer1 wrote:I wonder whether this is why Dr Simka and many others are talking about infections?
It could be an issue like the findings of infection involved in atherosclerosis wall adhesions, in the brain issues where there might be a sclerosis formed from the immune system attempts to repair an infection of the capillary, and there is also the issue of back jets effecting the small passages of the capillaries as well?
Some bacteria like CPn love endothelial walls and macrophages as host cells!
I was on the ABX's protocol for 12 months, and still have MS symptoms, and had the leg-pain-swelling thing, and had CCSVI.
Hi Cure,
from what I have heard there are many versions of the Protocol and different drugs used, there is also a time factor for treatment and some are requiring being on the protocol for a long time, as Sean T in Aust is finding at the moment with 22 months and still having herx reactions and no active MRI findings.
If we have been on DMD's then the bacteria will have modified and also hibernate when necessary to avoid treatments so we are assuming allot when we say that the protocol didn't work or I have no bacterial symptoms. Even a change of diet and stresses will have effects both positive and negative.
The combinations of stealth bacteria and the bio-films they live amongst is another problem with treatment.
The leg problems that you are having sound like it may be a separate yet similar issue regarding blood return, if both brain and leg are creating symptoms. I sometimes think that the Vascular search is to simplistic and the Dr's need to think outside the box more.
The tests that are done in a standard fashion will only find the standard issues and we with MS symptoms are not standard patients in the search for Vascular answers!
The placebo theory with PTA was also disproved by BNAC with their recent sham trial, both with those 50% treated and those not treated had NO symptom improvement and the 75% or better phase 1 arm HAD improvements, so imo that rules out PTA placebo!
Many people who have had MS PTA go on to have Leg vein PTA as well.
;)
Nigel
I disagree with you, nigel.
Both placebo and nocebo may have been at play in their reported outcomes.
However we still need to review this paper after it has undergone peer review in order to make any conclusions about why their results are so negative.
DrS
Re: DrSclafani answers some questions
Posted: Wed May 08, 2013 12:52 pm
by NZer1
I disagree with you, nigel.
Both placebo and nocebo may have been at play in their reported outcomes.
However we still need to review this paper after it has undergone peer review in order to make any conclusions about why their results are so negative.
DrS
Placebo and Nocebo, (and little lambs eat ivy) have peer reviewed figures from research on Placebo effect in MS and is 30-3% and this difference does not feature in the figures from BNAC.
So does mean you know something we don't, or does it mean that the figures from BNAC should not be trusted?
It was a small study correct, and 30% would feature if there was an outcome that improved the flow even in such a small study, like the wild card figure of one patient having several relapses has shown as a statistical observation.
If anything the printed 'opinions' from the study by BNAC staff have challenged the integrity of the study, imo.
Nigel
Re: DrSclafani answers some questions
Posted: Wed May 08, 2013 8:43 pm
by drsclafani
NZer1 wrote:
I disagree with you, nigel.
Both placebo and nocebo may have been at play in their reported outcomes.
However we still need to review this paper after it has undergone peer review in order to make any conclusions about why their results are so negative.
DrS
Placebo and Nocebo, (and little lambs eat ivy) have peer reviewed figures from research on Placebo effect in MS and is 30-3% and this difference does not feature in the figures from BNAC.
So does mean you know something we don't, or does it mean that the figures from BNAC should not be trusted?
It was a small study correct, and 30% would feature if there was an outcome that improved the flow even in such a small study, like the wild card figure of one patient having several relapses has shown as a statistical observation.
If anything the printed 'opinions' from the study by BNAC staff have challenged the integrity of the study, imo.
Nigel
trying to review a manuscript without reading it is unfair to the authors. How can you challenge the integrity without knowing the details?
Re: DrSclafani answers some questions
Posted: Wed May 08, 2013 10:37 pm
by NZer1
The way I understand the situation the BNAC team have made available a document that is for public awareness of their study and their opinions have been made in the press as well.
I have the opinion that it is open for comment if they have offered their work to conferences and media.
BNAC have made public presentations previously of their plan to inform in a transparent manor, at another presentation, so I am wondering why they have now presented two opinions publicly that don't match the details of their study purpose.
Nigel
Re: DrSclafani answers some questions
Posted: Thu May 09, 2013 3:32 am
by drsclafani
NZer1 wrote:The way I understand the situation the BNAC team have made available a document that is for public awareness of their study and their opinions have been made in the press as well.
I have the opinion that it is open for comment if they have offered their work to conferences and media.
BNAC have made public presentations previously of their plan to inform in a transparent manor, at another presentation, so I am wondering why they have now presented two opinions publicly that don't match the details of their study purpose.
Nigel
Nigel, the authors commenting on an abstract is quite different from the actual details of their work. Of course comments about the abstract and their commentary is fair game but the real devil is in the detail of the actual paper. Among the possibilities, as unlikely as it may be, is that peer review rejects this paper because of bad design. We must be patient.
Re: DrSclafani answers some questions
Posted: Thu May 09, 2013 11:15 am
by NZer1
Thanks Sal, appreciate you knowledge
Nigel
Re: DrSclafani answers some questions
Posted: Tue May 14, 2013 1:30 pm
by David1949
Dr. Sclafani
Do you know if eyelids are protected by the blood brain barrier? Two years ago I was on Doxycyclene which solved a problem I had with my eyelids. Other antibiotics didn't fix that. As far as I know Doxycyclene is one of only a few antibiotics that can get past the blood brain barrier.
Sorry if this isn't right up your alley, but I think you are probably better qualified to answer that than anyone else around here.
Re: DrSclafani answers some questions
Posted: Sun May 19, 2013 5:02 pm
by drsclafani
David1949 wrote:Dr. Sclafani
Do you know if eyelids are protected by the blood brain barrier? Two years ago I was on Doxycyclene which solved a problem I had with my eyelids. Other antibiotics didn't fix that. As far as I know Doxycyclene is one of only a few antibiotics that can get past the blood brain barrier.
Sorry if this isn't right up your alley, but I think you are probably better qualified to answer that than anyone else around here.
David, the eyelids are not part of the blood brain barrier. what was the problem that you encountered with your eyelids?
I was always thinking about the ways to examine the ccsvi caused by muscles' pressure
You've had some cases in the past, and you also mentioned the possibility of botox injection
Is there any test apart from angiogram one could have to see if there's a muscle compression on the jugulars?
Re: DrSclafani answers some questions
Posted: Tue May 21, 2013 5:38 pm
by David1949
drsclafani wrote:
David1949 wrote:Dr. Sclafani
Do you know if eyelids are protected by the blood brain barrier? Two years ago I was on Doxycyclene which solved a problem I had with my eyelids. Other antibiotics didn't fix that. As far as I know Doxycyclene is one of only a few antibiotics that can get past the blood brain barrier.
Sorry if this isn't right up your alley, but I think you are probably better qualified to answer that than anyone else around here.
David, the eyelids are not part of the blood brain barrier. what was the problem that you encountered with your eyelids?
Dr. Sclafani
Thank you for your reply. I had two prolems; 1) a chalazion which did not go away even after it was lanced by an opthalmologist. 2) redness and scaliness in the margin of the eyelids at the base of the lashes. Both problems went away after 1 month on Doxycycline. I think it's one of the few antibiotics than can get past the blood brain barrier.
Re: DrSclafani answers some questions
Posted: Tue May 21, 2013 6:48 pm
by drsclafani
David1949 wrote:
drsclafani wrote:
David1949 wrote:Dr. Sclafani
Do you know if eyelids are protected by the blood brain barrier? Two years ago I was on Doxycyclene which solved a problem I had with my eyelids. Other antibiotics didn't fix that. As far as I know Doxycyclene is one of only a few antibiotics that can get past the blood brain barrier.
Sorry if this isn't right up your alley, but I think you are probably better qualified to answer that than anyone else around here.
David, the eyelids are not part of the blood brain barrier. what was the problem that you encountered with your eyelids?
Dr. Sclafani
Thank you for your reply. I had two prolems; 1) a chalazion which did not go away even after it was lanced by an opthalmologist. 2) redness and scaliness in the margin of the eyelids at the base of the lashes. Both problems went away after 1 month on Doxycycline. I think it's one of the few antibiotics than can get past the blood brain barrier.
Sounds like your condition is related to oil glands in the skin. doxycycline supposedly affects this in a therapeutic way. I do not think that doxy only works by crossing the BBB. glandular problems. Some infections are sensitive to doxy when others do not have the desired effect.
You are absolutely correct though, This is not my expertise.
I was always thinking about the ways to examine the ccsvi caused by muscles' pressure
You've had some cases in the past, and you also mentioned the possibility of botox injection
Is there any test apart from angiogram one could have to see if there's a muscle compression on the jugulars?
pelopidas, some of these muscles are very nicely seen by sonography and by MRI. zamboni was discussing this recently in a case report.
but i need better evidence before I would recommend surgical release of muscles. This is not intuitive and it is phasic. I like the possibility of using botox as a provocative test of effect of release of the muscle. wish i knew how to use botox
a very difficult issue and one that needs some minds coming together to address.
Re: DrSclafani answers some questions
Posted: Tue May 21, 2013 7:59 pm
by drsclafani
NHE wrote:
miri wrote: OK, I finally checked them out, and I vote most for Rogan's video's since they quickly explain to novices what it's all about. Granted the others are amazing before-and-after's... but I was seeking more in the line of a quick education.
Hey, even Rogan's could have been condensed by a professional into one shorter video showing the "meat" of the matter. To give an unrelated example, I think the below parchment-cone video is better than the more-popular parchment-cone video's, since it offers "instant yet concise education" - see what i mean?
I doubt that you're ever going to find a step-by-step "do it yourself at home" CCSVI video. Instead, read some of Dr. Sclafani's several case study posts. These are a invaluable resource for people wishing to learn about CCSVI.
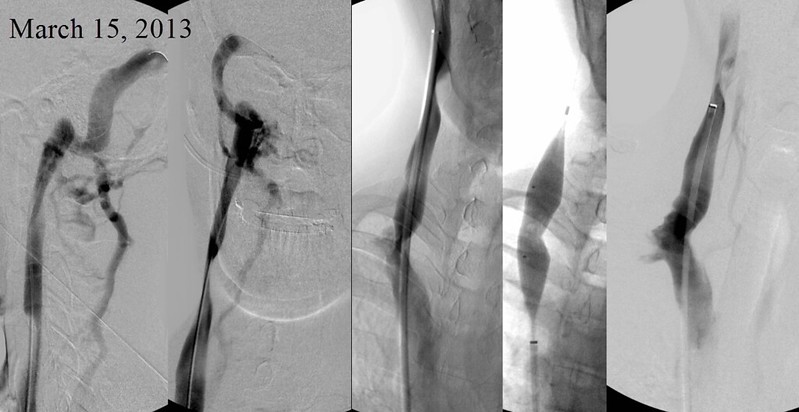
Thanks for the compliment. It deserves a response and here is an interesting case from this past week.
A 35 year old Canadian man with a rather aggressive form of RRMS resulting in cognitive dysfuction, memory difficulties, weakness and spasticity, fatigue, terrible imbalance, heat intolerance, depression.
He was seen by me in March 2013 where ultrasound revealed hemodynamic abnormalities on doppler that were consistent with CCSVI and thickened elongated immobile valves by Bmode ultrasound.
He underwent venography.
RIGHT INTERNAL JUGULAR VENOGRAPHY
Right sided venography (shown) and IVUS demonstrated about 95% internal jugular valvular stenosis, and compression stenosis of the mid-jugular vein. The valve stenosis was treated with a 20 mm high pressure balloon. The final image after several angioplasties looked pretty good to me.
LEFT INTERNAL JUGULAR VENOGRAPHY
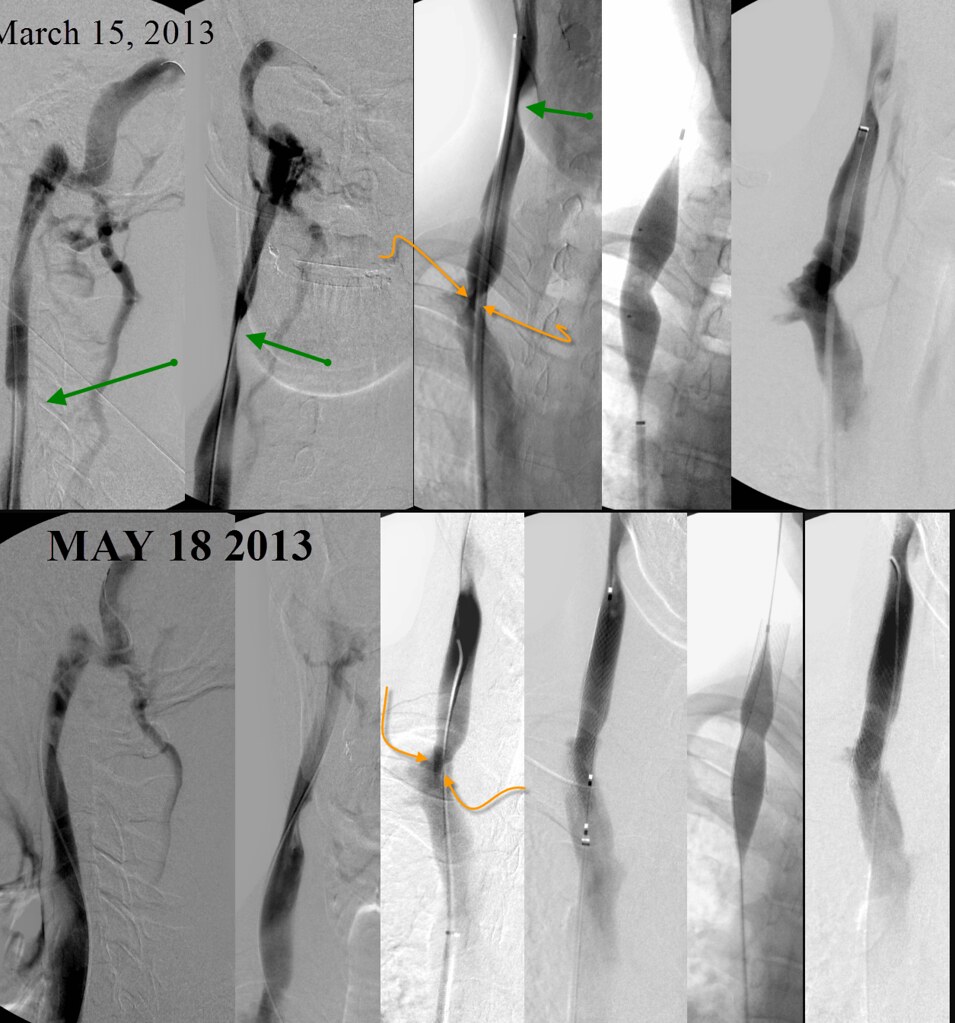
Left internal jugular venography revealed a similar valvular stenosis (orange arrows) as well as a stenosis from muscular compression (green circles).
The valvular stenosis was treated with a 16 mm high pressure balloon angioplasty. The compression stenosis was not treated. Endovasccular treatment of external compression would require stenting and I am reluctant to implant a permanent device for a phasic lesion that may not be significant This is certainly a hot topic of the moment but there is little clarity.
The patient had rather immediate, rapid and dramatic improvements in all of his symptoms. We were quite pleased. However after one week symptom improvements regressed rather quickly back to his baseline condition.
My advice was to "stay the course" , see if improvements returned. But they did not. All gains were lost.
The possible explanations are many:
Was this a short lived placebo effect?
Was something missed?
Did he have a relapse?
Did he thrombose a jugular?
Did he have restenose his valves?
Was he a non-responder?
Obviously, the most urgent consideration was thrombosis. Reversal of thrombosis requires rapid response to recanalize the occluded bein before the clot turned into scar tissue. Thankfully, ultrasound did not show any evidence of thromosis. However ultrasound showed abnormal valves and reflux.
We had some difficulty coordinating a return visit but the patient was seen again at two months after procedure. Venography was performed again, with completion of venography of both dural sinuses, jugular veins, brachiocephalic veins, the azygos vein, the left renal vein, the ascending lumbar vein and the inferior vena cava.
LEFT INTERNAL JUGULAR VEIN:
As you can see, the stenosis of the internal jugular valve has recurred.
RIGHT INTERNAL JUGULAR SYSTEM:
Similarly recurrent stenosis of the right valvular aparatus was quite apparent and significant.
Generally, I prefer to give angioplasty a second try as the next manuever. I prefer to withhold stenting after the first restenosis because some patients respond quite nicely to a second angioplasty and stenting can be avoided. The patient was quite concerned about repeated trips to New York City since his brother lived much further from new york and this was an impractical solution. Therefore I agreed to stent if restenosis was found.
I did not want to stent both sides so I thought to stent the most narrowed and larger vein and treat the other vein with simple angioplasty.
Therefore I treated the left side by repeat angioplasty and stented the right internal jugular vein using a Wallstent.
I do not have any good explanation why the effects of this patient's angioplasty proved to be so short lived. Perhaps the valve was incompletely opened the first time. perhaps it was just too thick to stay open. I must reveal that even after placement of the stent, balloon angioplasty had to be performed to get the valves to open completely.
I wait very impatiently to learn whether stenting of recurrent stenosis has been helpful.