Page 199 of 320
Re: CCSVI and CCVBP
Posted: Fri Apr 19, 2013 9:53 am
by costumenastional
Hello people! Here I am again. Neurological problems are not so rare these days, wouldn't you say?
Well, my mother is in trouble this time and I must admit that it is hard for me to see her having neurological symptoms. Very hard.
I believe the only thing that can help her is upper cervical care. And that's why I m here.
Happy to see you all again. We ll be in touch.
Re: CCSVI and CCVBP
Posted: Fri Apr 19, 2013 10:28 am
by uprightdoc
CN just updated me on his mother's history. She is 56 years old. Her problems began about five years ago. It started with pain in the foot. The foot pain later progressed to involuntary kicking. They thought it was due to an emotional response to stress at the time. A couple of years ago it turned into a footdrop. For the last year she was unable to walk without assistance. She also has numbness and weakness in her hands, as well as other symptoms that CN says don't bother her as much. I don't know what those symptoms are yet. In addition to her neurological complaints, she has neck pain and stiffness with decreased range of motion turning her neck while sitting.
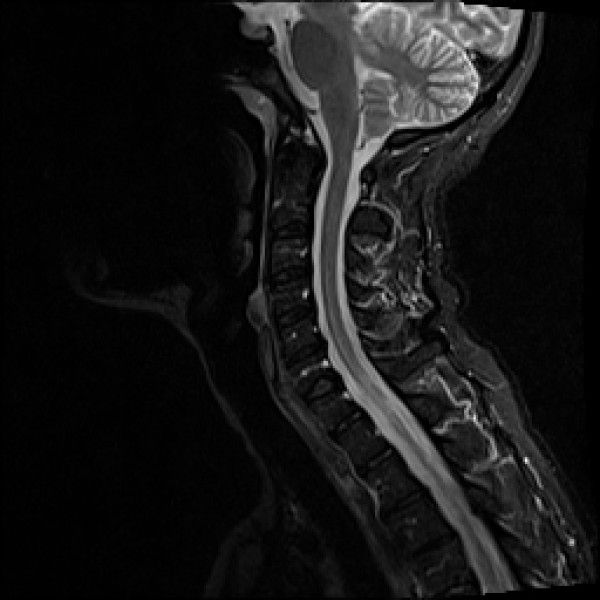
If you look at the scan closely you will see that the space beneath the cerebellum is very small. If you look to the right of the round looking portion of the cerebellum at the bottom you will see a bright white spot. That bright spot is bone. It is the rear side of the foramen magnum. The front of the foramen magnum is just across from it. In this image it appears that the lower portion of the cerebellum, called the tonsils, has descended somewhat, albeit slightly, into the foramen magnum. Technically, it is called cerebellar tonsilar ectopia. It should be noted, however, that this image was taken supine and that the degree of descent most likely increases in upright posture. CTE can compress blood and CSF pathways between the cranial vault and spinal canal. It can also increase pressure on motor and sensory tracts of the brainstem and cord in the foramen magnum and upper cervical canal.
Re: CCSVI and CCVBP
Posted: Fri Apr 19, 2013 11:21 am
by HappyPoet
CN, I'm sorry to hear about your mother and hope she feels better soon. Thanks very much for sharing her image, which when combined with DrF's terrific explanation, gives us a great learning experience. Thanks very much to you, too, DrF--I now understand much better CTE. Could CTE create chronic inflammation due to chronic compression and pressure? Thank you.
Re: CCSVI and CCVBP
Posted: Fri Apr 19, 2013 12:37 pm
by uprightdoc
Your welcome Poet and thank-you CN for sharing so others can learn. In answer to your question Poet, chronic compression and increases in pressure in the foramen and upper canal can cause ischemia, inflammation and edema. Chronic ischemia, inflammation and edema can be destructive to the brain and cord. In this case the ischemia, inflammation and edema is occuring in the cord. Hopefully, there hasn't been permanent damage and it can be turned around. The good news is her neck pain subsides following upper cervical correction using the Kale Specific Upper Cervical. That's a good sign. Improvement in range of motion is another good sign to monitor. In addition to correction, I would use ice, EMS, or US on a case like this along with TCMs to improve blood and CSF flow in the cord, as well as for reducing inflammation.
Re: CCSVI and CCVBP
Posted: Fri Apr 19, 2013 12:40 pm
by costumenastional
Re: CCSVI and CCVBP
Posted: Fri Apr 19, 2013 2:18 pm
by centenarian100
Location of the cerebellar tonsils < 3mm below the foramen magnus ("benign tonsillar ectopia") is normal
source:
http://radiopaedia.org/articles/chiari-i-malformation
This is a very common incidental finding. The MRI posted reveals a large amount of T2 bright CSF around the upper cervical cord, cerebellum, and brainstem. There is a no syrinx or brainstem compression
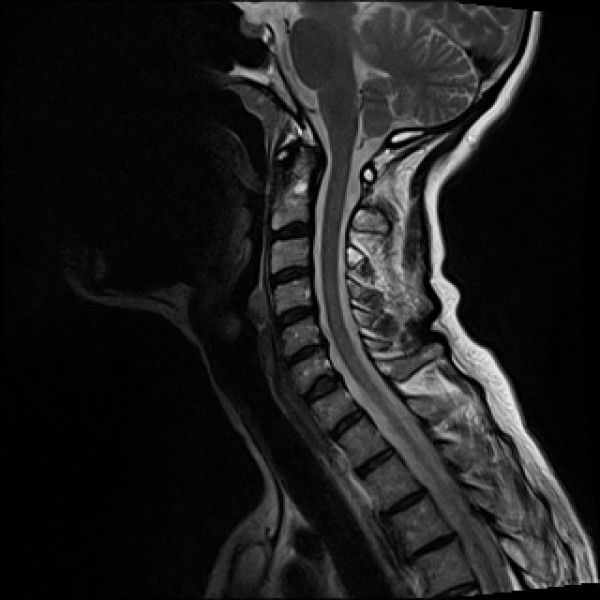
Here is what cerebellar tonsilar herniation looks like:

Although, it is possible for minimal tonsilar ectopia to be associated with some chiari malformation related symptoms: (
http://radiology.rsna.org/content/245/2 ... l.pdf+html)
Re: CCSVI and CCVBP
Posted: Fri Apr 19, 2013 6:01 pm
by HappyPoet
uprightdoc wrote:If you look at the scan closely you will see that the space beneath the cerebellum is very small. If you look to the right of the round looking portion of the cerebellum at the bottom you will see a bright white spot. That bright spot is bone. It is the rear side of the foramen magnum. The front of the foramen magnum is just across from it. In this image it appears that the lower portion of the cerebellum, called the tonsils, has descended somewhat, albeit slightly, into the foramen magnum. Technically, it is called cerebellar tonsilar ectopia. It should be noted, however, that this image was taken supine and that the degree of descent most likely increases in upright posture. CTE can compress blood and CSF pathways between the cranial vault and spinal canal. It can also increase pressure on motor and sensory tracts of the brainstem and cord in the foramen magnum and upper cervical canal.
Thanks, Dr. Flanagan,
You make an excellent point about supine versus upright imaging. My next set of MRIs will be in a FONAR Upright MRI machine--in fact, it will be the same machine I was in when I participated in Dr. Rosa's earlier clinical trial. Am still eagerly awaiting the published results from his latest study. Along with compression of arteries, veins, and nerves, turbulent CSF back-jets into my brain due to a misaligned C1 is something I want to avoid, so I continue to have my Atlas adjusted whenever necessary.

Edit: Fixed quote-I originally used the wrong one.
Re: CCSVI and CCVBP
Posted: Fri Apr 19, 2013 11:36 pm
by NZer1
centenarian100 wrote:Location of the cerebellar tonsils < 3mm below the foramen magnus ("benign tonsillar ectopia") is normal
source:
http://radiopaedia.org/articles/chiari-i-malformation
This is a very common incidental finding. The MRI posted reveals a large amount of T2 bright CSF around the upper cervical cord, cerebellum, and brainstem. There is a no syrinx or brainstem compression
Here is what cerebellar tonsilar herniation looks like:
Although, it is possible for minimal tonsilar ectopia to be associated with some chiari malformation related symptoms: (
http://radiology.rsna.org/content/245/2 ... l.pdf+html)
Hi centenarian 100, quick question will the Upright MRI findings be identical to supine MRI findings?
I ask because if they are the same, the standard MRI would be considered 'Gold Standard' for Neurological dx's, I would imagine, BUT if the findings are different then the Medical World would be .................
;)
Nigel
Re: CCSVI and CCVBP
Posted: Sat Apr 20, 2013 2:01 am
by uprightdoc
As I have mentioned many times on this thread -
it's not the degree of descent that matters. What matters is whether or not it causes problems. The signs and symptoms of Chiari 0 and Chiari 1 are similar to MS. In this case, CN's mother has classic symptoms of a Chiari malformation and classic signs of Chiari 0 or a Chiari 1 on supine MRI. The degree of descent will increase in the upright position. If it looks like a duck and quacks like a duck it probably is a duck.
The links below are to Chiari sites. The term Chiari 0 is used to describe zero or minimal descent with a syrinx in the cord.
http://www.csfinfo.org/node/179
http://www.wichiaricenter.org/oth/Page. ... =OTH000006
http://www.webmd.com/migraines-headache ... tion-10486
Re: CCSVI and CCVBP
Posted: Sat Apr 20, 2013 2:06 am
by uprightdoc
NZer1 wrote:... Dr F do you know a Dr David Jernigan? I am not sure if he studied at Sherman but he is a Chiro in Kansas...
NZer,
I don't know Dr. Jernigan and I didn't see anything about the doctor on the link you posted.
Re: CCSVI and CCVBP
Posted: Sat Apr 20, 2013 11:46 am
by NZer1
Thanks Dr F I have since found out he was at Cleveland.
I am trying to 'profile' his methods for Lyme disease and see what credentials he has. He has posted on his FB site some good threads and I have read his book on Lyme and Bacterial infections.
All my studies at the moment seem to be hovering around the bacterial diseases and looking at the symptom links with de-generative diseases.
Take care everyone
;)
Nigel
Re: CCSVI and CCVBP
Posted: Sun Apr 21, 2013 1:32 am
by NZer1
I was talking to Franz Schelling earlier today and a couple of examples came up in conversation that I think are of interest here as well (Thanks to Franz)
Abstract
PRIMARY OBJECTIVE:
Chiari malformation is defined as herniation of the cerebellar tonsils through the foramen magnum, also known as cerebellar tonsillar ectopia (CTE). CTE may become symptomatic following whiplash trauma. The purpose of the present study was to assess the frequency of CTE in traumatic vs non-traumatic populations.
STUDY DESIGN:
Case-control.
METHODS AND PROCEDURES:
Cervical MRI scans for 1200 neck pain patients were reviewed; 600 trauma (cases) and 600 non-trauma (controls). Half of the groups were scanned in a recumbent position and half were scanned in an upright position. Two radiologists interpreted the scans for the level of the cerebellar tonsils.
MAIN OUTCOMES AND RESULTS:
A total of 1195 of 1200 scans were read. CTE was found in 5.7% and 5.3% in the recumbent and upright non-trauma groups vs 9.8% and 23.3% in the recumbent and upright trauma groups (p = 0.0001).
CONCLUSIONS:
The results described in the present investigation are first to demonstrate a neuroradiographic difference between neck pain patients with and without a recent history of whiplash trauma. The results of prior research on psychosocial causes of chronic pain following whiplash are likely confounded because of a failure to account for a possible neuropathologic basis for the symptoms.
http://www.ncbi.nlm.nih.gov/pubmed/20545453
and
The spinal cords were examined in eighteen cases of multiple sclerosis, with special attention to the cervical enlargement. It was found that (1) lesions in the cervical cord are about twice as common as at lower levels, (2) in this region there is a striking preponderance of fan-shaped lesions in the lateral columns. It is argued that both these findings are explicable on the theory that mechanical stresses play a part in determining the site of lesions; that such stresses are commonly transmitted to the cord via the denticulate ligaments during flexion of the spine; and that many of the lesions are attributable to vascular leakages due to tension in the denticulate ligaments. It is concluded that in patients with multiple sclerosis neck flexion is dangerous–especially in cases where Lhermitte's sign has occurred.
http://onlinelibrary.wiley.com/doi/10.1 ... x/abstract
Nigel
Re: CCSVI and CCVBP
Posted: Sun Apr 21, 2013 10:14 am
by costumenastional
Thanks Nigel.
Re: CCSVI and CCVBP
Posted: Mon Apr 22, 2013 11:24 am
by centenarian100
NZer1 wrote:Hi centenarian 100, quick question will the Upright MRI findings be identical to supine MRI findings
not necessarily:

source:
http://www.conquerchiari.org/subs%20onl ... 06(2).html

The authors describe cases of people with "occipitoatlantoaxial hypermobility" and sometimes clinical symptoms of brainstem dysfunction in upright position.
Re: CCSVI and CCVBP
Posted: Mon Apr 22, 2013 11:29 am
by centenarian100
uprightdoc wrote:As I have mentioned many times on this thread - it's not the degree of descent that matters. What matters is whether or not it causes problems.
fair enough, but her symptoms are not suggestive of Chiari-related symptoms.
Did she describe postural posterior headaches or cerebellar dysfunction or anything typically associated with Chiari-I? You want to attribute her foot drop to <3mm of cerebellar herniation?
uprightdoc wrote: The signs and symptoms of Chiari 0 and Chiari 1 are similar to MS.
Not really