Page 1 of 7
DrSclafani dialogues w other doctors re:CCSVI interventions
Posted: Tue Jan 11, 2011 11:44 pm
by drsclafani
We know there are lurking physicians out there who are curious, learning, trying to get a handle on this liberation thing. Perhaps you are an interventionalist. Perhaps a surgeon, perhaps a physician patient, perhaps a neurologist or family practioner. You know who you are. I know who some of you are. its time to come in, take off your coat and join a physician discussion.
I cant promise that the patients won't join in but i ask them to lurk for a change. Perhaps they will learn by hearing our points of views. We all know we came here because we wanted to learn their points of view.
This is the new era of internet dialogue. Patients, most keenly interested in understanding THEIR disease and its consequences and cures, have driven this. They have brought information to me and you. This exchange is most healthy. Witness the thread on patient symptoms of the last couople of weeks. I have learned and my patients shake their heads affirmatively. "yes, it is like moving your hand in cool molasses"
This way of doing our business has merit. Its not peer reviewed but peer review is discussed. I have been here teaching for almost a year. And 50,000 views per month mean that someone is learning something. It's time for more points of view.
I consulted Jimmylegs. Her view was that all are invited to TIMS. As long as the rules are followed. So give yourself a moniker, and jump in the pool. The water is mostly warm and sometimes hot.
So I would like to hear from some of you. Lets show the patients that we care and that we struggle on the edge for them.
Posted: Wed Jan 12, 2011 5:24 am
by uprightdoc
Hello Dr. Scalfani,
I just recieved a post from Frodo inviting me to join your thread so here I am. My background is in chiropractic, neurology and physical anthropology as it pertains to the unique design of the skull, spine and circulatory system of the brain and cord due to upright posture.
Dr. Flanagan
Posted: Wed Jan 12, 2011 1:04 pm
by jimmylegs
clarification: *her* point of view

Posted: Wed Jan 12, 2011 1:12 pm
by drsclafani
jimmylegs wrote:clarification: *her* point of view
are you a physician?

Posted: Wed Jan 12, 2011 2:30 pm
by DrCumming
subscribing
Posted: Wed Jan 12, 2011 4:01 pm
by jimmylegs
I consulted Jimmylegs. His view was that all are invited to TIMS.
CASE STUDY #1
Posted: Wed Jan 12, 2011 11:00 pm
by drsclafani
So let's see who come out of the closet!
rule 1: we stay on this case until there are no responses for 24 hours
rule 2. one case discussion at a time
rule 3. patients lurk, comments only by doctors
here goes
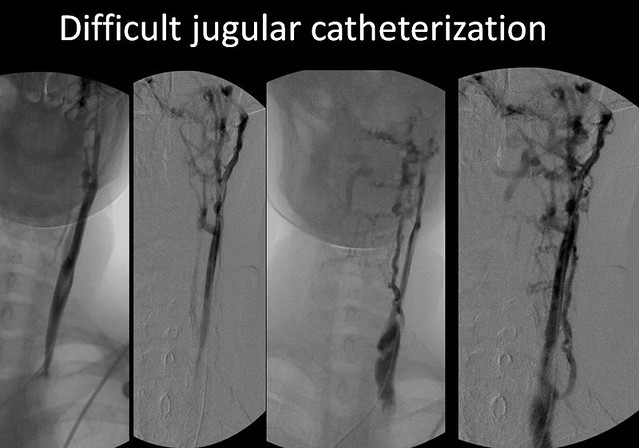
The patient is a 33 year old female with short term memory deficiencies, cognitive dysfunction, fatigue, headaches, and imbalance. She has numbness in both hands and the soles of both feet and temperature intolerance. Weakness is predominantly in the lower extremities. She has moderate spasticity, which is worse in the morning. She has co-morbidities of rheumatoid arthritis and multiple sclerosis.
Doppler and B-mode ultrasound of the neck in supine and erect positions and transcranial doppler of the deep cerebral veins was positive for more than one criteria and consistent with CCSVI.
Venography was performed via a left femoral approach.


[/img]
what is your interpretation?
What would be your next step?
Re: CASE STUDY #1
Posted: Thu Jan 13, 2011 3:07 am
by phlebologist
drsclafani wrote:
The patient is a 33 year old female with short term memory deficiencies, ......... what is your interpretation?
What would be your next step?
Right internal jugular vein - most likely normal, assuming that the outflow was good (this will be better visible in the movie than in a single picture) and neither Doppler ultrasound not MRV were predictive of a pathology
Left internal jugular vein - stenosis in the area of valve (junction with brachiocephalic vein); on the pictures collateral outflow is visible and also the valve seems to be stenotic (again, it should be better visible in the movie); left IJV has smaller diameter than right IJV, but it is a very common situation, not a pathology
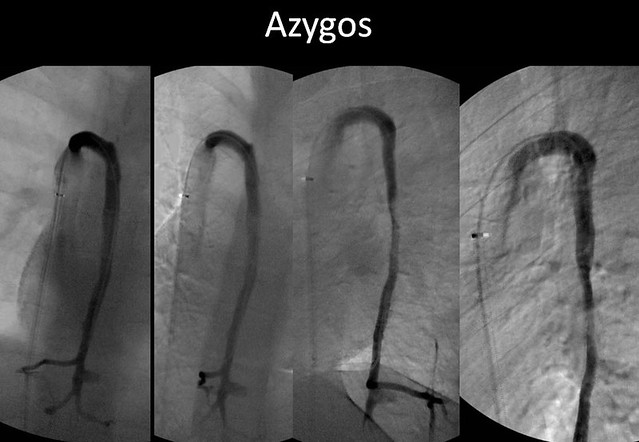
Azygous vein - seems to be normal
Proposed treatment - left IJV: balloon angioplasty of the area of valve; no stenting, at least - not during the first procedure, perhaps cutting balloon will be needed if the stenosis would not respond to ballooning
Lurking Pharmacist
Posted: Thu Jan 13, 2011 3:39 am
by MarkW
Hello Prof S,
Great idea for a thread, I hope patients just lurk.
With both MS and RA your young lady is likely to taking a cocktail of medication, given both from her several doctors and herself. Suggest an MUR (medicine use review). Also she may have unusual clotting times from her conditions/meds.
A MAB (used for RA) is being tested in pwMS so could be worth considering after de-stenosis. Your patient could get a double benefit. However the MAB has a 6-12 month dose scheme so not a simple decision.
Sounds like a case conf is needed, then a case study for a keen young doctor ?
Is checking the ascending lumber vein part of the latest diagnosis ?
Kind regards,
MarkW
PS I suggest the 'L' word is only used to provoke neuros deliberately. I have been de-stenosed but still have MS.
Re: CASE STUDY #1
Posted: Thu Jan 13, 2011 5:35 am
by uprightdoc
drsclafani wrote:The patient is a 33 year old female with short term memory deficiencies, cognitive dysfunction, fatigue, headaches, and imbalance. She has numbness in both hands and the soles of both feet and temperature intolerance. Weakness is predominantly in the lower extremities. She has moderate spasticity, which is worse in the morning. She has co-morbidities of rheumatoid arthritis and multiple sclerosis.
Doppler and B-mode ultrasound of the neck in supine and erect positions and transcranial doppler of the deep cerebral veins was positive for more than one criteria and consistent with CCSVI.
Venography was performed via a left femoral approach.
what is your interpretation?
What would be your next step?
I see a significant head and neck tilt to the left, which is the same side as the stenotic left IJV. The head tilt may be the cause or a contributing factor to compression of the left IJV. I also see a thoracolumbar scoliosis with significant pelvic tilt and leg length discrepancy.
I would order specific upper cervical x-rays using sterotaxic head clamps to include AP and Lat cervicals, OMO (or nasium) and vertex or base posterior views of the FM and spinal canal. I would also order AP and lateral lumbar x-rays and if possible a 14x36 AP full spine. Based on the findings of the plain view x-rays I would also consider a cervical MRI to rule out spondylosis and stenosis.
For patient care, I would recommend the patient undergo specific upper cervical intervention and follow-up cervical and transcranial ultrasound and doppler scans. I would co-manage the case with a neurologist to monitor the neurological signs and symptoms.
Correction of the upper cervical spine may help to improve circulation in the vertebral arteries, the vertebral veins, and the subarachoid space. It may also help to relieve mechanical compression of the internal jugulars and lengthen the durability of the angioplasty.
Re: CASE STUDY #1
Posted: Thu Jan 13, 2011 7:17 am
by drsclafani
phlebologist wrote:drsclafani wrote:
The patient is a 33 year old female with short term memory deficiencies, ......... what is your interpretation?
What would be your next step?
Left internal jugular vein - stenosis in the area of valve (junction with brachiocephalic vein); on the pictures collateral outflow is visible and also the valve seems to be stenotic (again, it should be better visible in the movie); left IJV has smaller diameter than right IJV, but it is a very common situation, not a pathology
phlebologist:
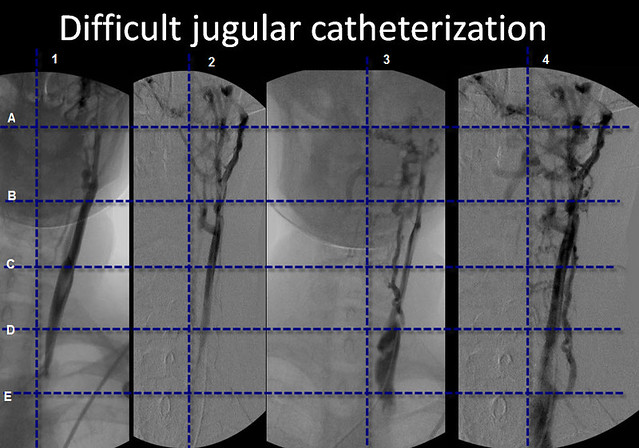
i agree that diameter of right and left ijv are common assymetrical. However, exactly which of these veins do you think is the LIJV. For more clarity among us, i would like some judgement about this. I have taken one of the images and put some grids on it. Would you all point to the closest intersections that show the LIJV
Re: CASE STUDY #1
Posted: Thu Jan 13, 2011 7:49 am
by drsclafani
uprightdoc wrote:drsclafani wrote:The patient is a 33 year old female with short term memory deficiencies, cognitive dysfunction, fatigue, headaches, and imbalance. She has numbness in both hands and the soles of both feet and temperature intolerance. Weakness is predominantly in the lower extremities. She has moderate spasticity, which is worse in the morning. She has co-morbidities of rheumatoid arthritis and multiple sclerosis.
Doppler and B-mode ultrasound of the neck in supine and erect positions and transcranial doppler of the deep cerebral veins was positive for more than one criteria and consistent with CCSVI.
Venography was performed via a left femoral approach.
what is your interpretation?
What would be your next step?
I see a significant head and neck tilt to the left, which is the same side as the stenotic left IJV. The head tilt may be the cause or a contributing factor to compression of the left IJV. I also see a thoracolumbar scoliosis with significant pelvic tilt and leg length discrepancy.
I would order specific upper cervical x-rays using sterotaxic head clamps to include AP and Lat cervicals, OMO (or nasium) and vertex or base posterior views of the FM and spinal canal. I would also order AP and lateral lumbar x-rays and if possible a 14x36 AP full spine. Based on the findings of the plain view x-rays I would also consider a cervical MRI to rule out spondylosis and stenosis.
For patient care, I would recommend the patient undergo specific upper cervical intervention and follow-up cervical and transcranial ultrasound and doppler scans. I would co-manage the case with a neurologist to monitor the neurological signs and symptoms.
Correction of the upper cervical spine may help to improve circulation in the vertebral arteries, the vertebral veins, and the subarachoid space. It may also help to relieve mechanical compression of the internal jugulars and lengthen the durability of the angioplasty.
i think you are jumping to conclusions. During this procedure,, there was no focus upon the spine. The images were not taken with the patient in a position that would allow analysis of the spine, simply comfort. These images were not straight either, the C-arm was placed in a variety of positions and angulations. The images of the azygos vein, where one sees the thoracic spine, have subtracted out the bones and are done in 20, 70 and 90 degrees of angulation. I would be cautious about reading too much about scoliosis into such images.
Re: CASE STUDY #1
Posted: Thu Jan 13, 2011 8:36 am
by uprightdoc
drsclafani wrote:uprightdoc wrote:drsclafani wrote:
i think you are jumping to conclusions. During this procedure,, there was no focus upon the spine. The images were not taken with the patient in a position that would allow analysis of the spine, simply comfort. These images were not straight either, the C-arm was placed in a variety of positions and angulations. The images of the azygos vein, where one sees the thoracic spine, have subtracted out the bones and are done in 20, 70 and 90 degrees of angulation. I would be cautious about reading too much about scoliosis into such images.
Regardless of subtraction of the bones from the images the spine is still visible and shows abnormal curvatures. Unless taken to the extreme, positioning the patient for comfort won't significantly change scoliotic or kyphotic curvatures. Nor will raising the arm overhead cause a thoracolumbar scoliosis or curvature in the neck. In any case, plain view x-rays would be a safe, inexpensive and convenient way to find out if there are abnormal curvatures in the spine causing or contributing to the problem. Additionally the patient exhibits signs of vertebral-basilar artery insufficiency, which is why I recommend specific upper cervical x-rays to check the alignment of the upper cervical spine and neural canal.
Re: CASE STUDY #1
Posted: Thu Jan 13, 2011 8:48 am
by drsclafani
not a problem.we just strongly disagree
Re: CASE STUDY #1
Posted: Thu Jan 13, 2011 9:18 am
by uprightdoc
drsclafani wrote:uprightdoc wrote:drsclafani wrote:
I am not sure which part of what I said you strongly disagree with but at least we both agree that CCSVI plays a role in MS. My point is that the blood vessels follow the curves of the spine and curvatures of the spine have been shown to cause functional stenosis which, among other things, can affect venous flow in the VVP. Upper cervical misalignments can further lead to chronic craniocervical venous back pressure (CCVBP) against the brain. CCVBP also affects CSF pulsatility and flow.