Page 43 of 49
Posted: Wed Aug 10, 2011 3:01 am
by bluesky63
I absolutely have to weigh in on drinking a glass of water -- I was astounded to have this as an entirely unexpected benefit of venous angioplasty. I could drink a full glass of water, without stopping, for the first time in many years, where before I would just gasp through it. Along with that I could sing properly again.I think I mentioned this when I described my odd set of improvements immediately post-procedure because I didn't remember seeing it before, but now I've seen this pop up here and there!
I thought it might be an effect to the diaphragm since I also stopped having hiccups every single time I has sparkling water. Isn't it amazing?
Posted: Wed Aug 10, 2011 11:30 am
by Cece
Did it last, bluesky?
Back in February when I described my difficulties breathing when reading, Dr. Sclafani said it sounded like diaphragm spasms. I haven't had a chance to read up on that but it sounds like what you're suggesting too.
CD, it makes sense, and what a lot of lousy things we have to bear.
Posted: Wed Aug 10, 2011 12:00 pm
by Cece
Cece wrote:
Here is my dural sinus venogram on the right side....
I had previously said that my right side might be how the verts should look, since the other side showed them more prominently and the other side turned out to be 70% blocked down at the area of the valves.
But having gotten my three page report on the procedure in the mail, I stand corrected.
"[...] Examination began with the right transverse sinus. Dural venography demonstrated that that was patency of the right transverse and sigmoid sinuses. The jugular bulb was intact with no evidence of stenosis. Prominent posterior vertebral filling was noted."
skipping ahead to this:
"Selective catheterization of the left internal jugular vein was then performed. The catheter was positioned in the left transverse sinus. Dural venography again showed very prominent vertebral filling. However no evidence of stenosis in the dural sinuses or the bony jugular bulb was identified."
There is much more to the report that we can discuss. But it is of note that on both sides my verts were more prominently filling than would be expected.
Posted: Wed Aug 10, 2011 12:30 pm
by Cece

from the report of my July 11th 2nd procedure:
"The catheter was then withdrawn into the internal jugular vein and venography was performed. This revealed that there was slow flow exiting the internal jugular vein. There was some prominent distention at the J2 segment, but this rapidly came to an abrupt high-grade stenosis of about 70%. There is stasis within the jugular vein with reflux noted. Intravascular ultrasound showed that there was persistent transverse tissue band extending around the region of the valvular area."
Based on intravascular ultrasound, a 10-mm Diamond balloon was positioned in the region of the stenosis and inflated. This showed a tight narrowed annular constriction of the balloon, which resolved with 8 atmospheres of pressure. Repeat venography on IVUS showed continued transverse tissue bands as well as slow flow and persistent narrowing at the region of the valve. Therefore, a 12 mm x 4 cm long Atlas balloon was positioned in the region of the stenosis and inflated to 8 atmospheres. A waist was eliminated at 8 atmospheres. There was markedly improved flow through this vein at that time. Intravascular ultrasound still showed some band-like tissue. I elected to not inflating the larger balloons at this time."
I do not have the final IVUS image showing the band-like tissue. I wonder what that looks like on IVUS?
So, as I understand this, he ballooned with the 10 mm balloon and a waist was eliminated but the flow was still slow and the valve still narrowed. He ballooned with the 12 mm balloon and another waist was eliminated. What does it mean if two waists can be eliminated like that in the same location?
I think the fact that there was still residual band-like tissue is unfortunate. I wish my vein had cooperated fully. My husband weighed in on it with extreme gratitude that Dr. Sclafani did not balloon any further. "What if you lost the whole vein?" If caution might mean reduced durability, maybe, but aggression means increased risk of vein loss, I am definitely in the cautious camp. I've had benefits since this second procedure that I did not have the first time around. That left jugular matters.... (And I agree that there may be a "just-right" point, that Dr. Sclafani is trying to determine, somewhere in the middle of caution and aggression.)
Posted: Wed Aug 10, 2011 1:30 pm
by David1949
Cece wasn't it your right leg that suffered drop foot? That would fit with CCSVI in the left jugular, since the left side of the brain controls the right side of the body.
Posted: Wed Aug 10, 2011 2:53 pm
by Cece
I said the same thing about my left jugular having restenosed and the numbness being in my left arm but Dr. Sclafani is having none of that. He has not seen a link between side of jugular blockage and side of MS difficulties.
Of course I had bilateral jugular stenosis with both sides being pretty bad. My right dropfoot improved in May at a time when I think (but don't know) that my left jugular had already closed back up and my right jugular was open.
Posted: Sun Aug 14, 2011 6:51 pm
by Cece
Cece wrote: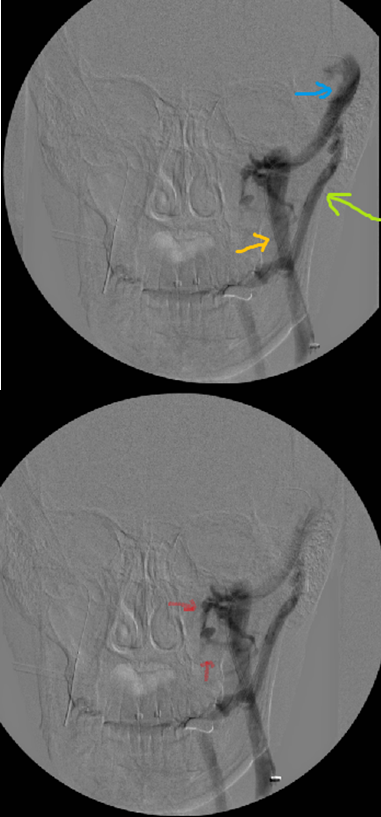
Cece wrote:almost forgot this one...

This is my left dural sinus from the side angle. The sinus itself looks healthy, as did the sinus on my right side. It is connected to the jugular as it should be.
Any questions? ;)
Does anything in there look like an enlarged hypoglossal emissary vein?
Posted: Sun Aug 14, 2011 7:49 pm
by drsclafani
Cece wrote:Cece wrote:
Cece wrote:almost forgot this one...
This is my left dural sinus from the side angle. The sinus itself looks healthy, as did the sinus on my right side. It is connected to the jugular as it should be.
Any questions? ;)
Does anything in there look like an enlarged hypoglossal emissary vein?
cecde
i have created confusion. i believe i have been corrected and agree that you have prominent condylar emissary veins.
Posted: Sun Aug 14, 2011 9:23 pm
by Cece
Thanks. I have not been familiar with the differences between hypoglossal and condylar emissary veins, only that they actually go through the skull.
Posted: Sun Aug 14, 2011 9:41 pm
by CD
Does the superior ophthalmic vein drain that way too? Could that be why vision changes are seen after the CCSVI procedure? Curious...
CD
Posted: Tue Aug 16, 2011 8:17 pm
by Cece
CD, I don't know. I thought the eye was drained by veins that drained into the internal jugulars. The emissary veins are tiny veins that contribute to the drainage of the venous dural sinuses. Emissary veins actually travel through the skull in little canals just for them, from what I understand. When I looked them up yesterday, I found some discussion that trauma can sever these emissary veins. Aha! I thought. Here is another explanation for patients who associate trauma with incipient MS symptoms.
Then I read that the severing of emissary veins leads to subdural hematoma, which is very serious and noticeable and can be fatal. So I took down a post I made here about it, actually.
Then I gave it more thought and I think, if these veins can be severed during trauma, they can also probably be injured to any degree up to the point of severing. So head trauma could cause these emissary veins to be damaged, but not altogether severed, which would lead to the blockage of these veins as a cerebrospinal route, which could worsen CCSVI, although I think these veins are too small to be contributing much to the flow.
There is also the earlier information that trauma to the head can cause shearing of neurons, which would worsen a condition that was perhaps borderline or subclinical MS, thus bringing it out into the open.
And since most people have a car accident or a bump to the head in their personal history, it could just be a coincidence of timing or a tendency of humans to attribute causality to randomness.
I am glad I have a whole thread of my own, it is good for rambles.

Posted: Tue Aug 16, 2011 9:11 pm
by NZer1
Cece, my interest in the passages through the skull was from the angle that can they can become enlarged. The flow through them does the enlargement. I don't know if that is violent flow or not, but regular flow that is greater than the diameter of the skull enlarges the passage. If the passage on one side is larger than its opposite there is most likely flow drainage issues on the opposite side of main flow (within the brain). How the blood flows within the brain is a whole story that hasn't seen the light of day and needs to be given total attention as much as CCSVI. We have no idea or understanding what is happening when the natural flow is changed, there must be portions of the brain that are unable to function in low oxygenated regions, hence the neuroplasticity action. The brain changes itself to achieve function in the available environment, same as in stroke patients.
My interest was that Dr. S had found an example of single enlarged passage and it was the first I had heard of on CCSVI threads.
ps did you get to read Dr. Flanagans book? Another great read is The Brain that Changes Itself by Norman Doidge, MD
All this adds to a picture when pieced together, and after reading Marie Rhodes and Terry Wahls books the importance of blood and its contents is in its infancy for us PwMSers.
Hope your well Cece,
Nigel
It seems that the flow can be hindered in many places on its travels. The challenge is to look everywhere and anywhere.
Posted: Tue Aug 16, 2011 9:11 pm
by CD
If not trauma, injury, vaccination or an illness, i.e. viral or bacterial, perhaps it is just congenital. We are born with minor or major defects in the veins. We have veins all over the body doing miracle jobs keeping us alive, arteries too.
We don't know what are bodies are like inside. It could be a jumble of errors and mismatches.
I am sure when a doctor opens a person up at autopsy, we have so many differences. We all must be unique on the inside.
Then add one of the incidents from above, and bingo CCSVI. What triggers CCSVI to activate? There will always be questions, theories and doubts. Then next it will be ,"Well, if that causes CCSVI?-what cures it? What cures it forever?
Is it a separate entity that just happens to help MS and other Neurological diseases?
Cece, when you think of head and brain injury, subdural bleeding, clotting or weakness, bulges, think also, of " Shaken Baby Syndrome."
Even just tossing a baby in the air to play with them, swinging them around like an airplane and they love it. There's always more than very severe trauma or head wound. It could be subtle, yet sickly or deadly years later.
Anyway, I still wonder about the eyes and their draining.
Late night rambling, my husband is on a trip.
CD
Re: Cece's turn
Posted: Fri Sep 09, 2011 6:47 am
by Cece
Today I have a doppler ultrasound appointment with Dr. Cumming here in Minneapolis. It's two months post-procedure and I've been doing very well. Let's hope that's reflected in two open, flowing, patent jugulars....
Re: Cece's turn
Posted: Fri Sep 09, 2011 10:08 am
by blossom
cece, hope all goes well for you.