Page 1 of 1
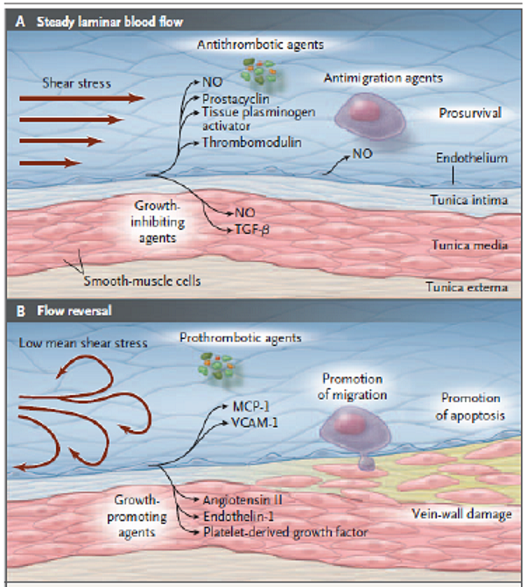
diagram for the effects of reversed blood flow
Posted: Fri Feb 25, 2011 7:19 am
by Cece
I found this really helpful, particularly after our discussions in the last few months of intimal hyperplasia, since what is going on when there is turbulent blood flow looks a lot like intimal hyperplasia even before any procedure is done:
It's from this URL but too small there:
http://tinyurl.com/6xzyw29
from this research article:
www.nejm.org/doi/full/10.1056/NEJMra055289
The top one is how the vein flow should be, the bottom one is us with our CCSVI veins. All those growth-promoting agents? That's the same as in intimal hyperplasia, the vein's response to injury, which is to grow thicker.
This is why I believe our CCSVI malformations are both malformations from birth (as agreed upon by the consensus of phlebologists) and that they worsen over time (as has shown up in imaging studies). CCSVI promotes the worsening of CCSVI.
I am not sure if the site of vein wall damage represents thickening or sloughing off of dead cells ("promotion of apoptosis.") But if it is vein wall damage, the body's response to vein wall damage is intimal hyperplasia, and the CCSVI stenosis would grow thicker.
"Promotion of migration" would be the increase in adhesion molecules and greater likelihood of white blood cells and who knows what making it past the blood brain barrier onto delicate tissue.
Posted: Fri Feb 25, 2011 7:46 am
by cheerleader
Great pics, Cece. They really illustrate the healing process. This is why an anticoagulant protocol, moderate exercise, hydration and anti-inflammatory diet and supplements are essential after treatment. It is the continued shear stress (literally, the healthy flow of blood against the vessel wall) that promotes endothelial healing. If there is hypercoagulation, excessive inflammation, hypovolemia (dehydration) or lack of shear stress, the endothelium is impaired. The blood flow doesn't need to be reversed to be damaging, merely being slow or not consistant enough can hurt as well. Shear stress is essential.
Simka's paper on shear stress
Aftercare is essential to venous health after angioplasty. I hope the doctors come up with a protocol. But for those wishing information for themselves, the endothelial health program points to the science behind all of this-
http://www.ccsvi.org/index.php/helping- ... ial-health
cheer
Posted: Fri Feb 25, 2011 9:49 am
by HappyPoet
Thank you, Cece and cheer -- it's research-backed threads/posts like these that have helped so many pwMS.
The pictures are terrific and really help me understand and appreciate what's happening inside the vein. I never knew that sheer stress is healthy and, indeed, necessary... so I plan to lay down as much as possible after my second procedure to give my veins the opportunity to properly heal -- I didn't know the importance of this after my first procedure when I often mistakenly slept in my recliner when I should have been on my bed.
Thank you again! Very much!
Posted: Fri Feb 25, 2011 5:01 pm
by frodo
Thanks Cece. This is the first time I find an explanation for the results of Zivadinov (vein problems worsen with time)
Posted: Sat Feb 26, 2011 10:40 am
by 1eye
This is why I believe our CCSVI malformations are both malformations from birth (as agreed upon by the consensus of phlebologists) and that they worsen over time (as has shown up in imaging studies). CCSVI promotes the worsening of CCSVI.
I agreed with you in "your" thread: not just because of these biochemicals, but because of sugar and oxygen! If there isn't enough to make a slow trip through the brain, that can't be healthy for the outflow pipes either.
Speaking of intimal hyperplasia and such, I have just finished re-recording a performance of Shakespeare's Hamlet. It occurred to me that maybe the multitudes of theories about Hamlet have left out possible circulation problems as a theory! Also, maybe he suspected there was madness in his method, and didn't want to pass on questionable genes, so that's why he blew off Ophelia.
Just a thought. Back to your buzz-groups...
Posted: Sat Feb 26, 2011 12:23 pm
by Cece
frodo wrote:Thanks Cece. This is the first time I find an explanation for the results of Zivadinov (vein problems worsen with time)
Yes, exactly. I'd heard this same concept that's shown in the images explained, but it's easier to see when you're seeing it than when reading, for me as well.
There's no reason to come up with some of the convoluted interpretations that we've read even in the research articles themselves, not when there's a simple explanation for why CCSVI would worsen over time to be found in the basic biological effects of the CCSVI itself disrupting the bloodstream.
1eye wrote:I agreed with you in "your" thread: not just because of these biochemicals, but because of sugar and oxygen! If there isn't enough to make a slow trip through the brain, that can't be healthy for the outflow pipes either.
Yes, I haven't read up too much on it, but the outer walls of the vein are surprisingly anoxic or low oxygen, and being too anoxic can again spur intimal hyperplasis regrowth. This is why placing a stent may be bad for the vein, because the stent may reduce the amount of oxygen that gets to the vein. Again, I haven't read enough on this to speak with confidence but I found it intriguing.
Posted: Sat Feb 26, 2011 12:40 pm
by pairOdime
They didn't have an explanation for the significantly elevated ET-1 levels in MS patients in 2001. It appears we now know the cause....CCSVI.
http://www.ncbi.nlm.nih.gov/pubmed/11315981
J Neuroophthalmol. 2001 Mar;21(1):37-8.
Increased endothelin-1 plasma levels in patients with multiple sclerosis.
Haufschild T, Shaw SG, Kesselring J, Flammer J.
University Eye Clinic, Basel, Switzerland.
OBJECTIVE: We tested the hypothesis that the plasma level of endothelin-1 (ET-1) is increased in patients with multiple sclerosis (MS). The peptide ET-1 is one of the most potent known vasoconstrictors. An increased level of endothelin could explain some of the vascular symptoms of these patients.
MATERIALS AND METHODS: A specific radioimmunoassay was used to determine ET-1 plasma levels. Twenty patients with MS were compared to 20 age- and sex-pair-matched healthy subjects.
RESULTS:
The plasma ET-1 levels were, on average, 224% higher in the patients with MS than in the controls (p < 0.005). The mean ET-1 levels (mean +/- standard deviation [SD]) were 3.5 +/- 0.83 pg/mL (min 2.13, max 5.37 pg/mL) in patients with MS and 1.56 +/- 0.3 pg/mL (min 0.9, max 2.13 pg/mL) in healthy volunteers.
Neither the different forms nor stages of MS had an influence on the results. The ET-1 level was also not correlated with the duration of the disease.
CONCLUSIONS:
The plasma ET-1 level is markedly and significantly increased in patients with MS. Neither the cause of such an increase nor the pathogenetic role is known.
Posted: Tue Apr 12, 2011 12:46 pm
by Cece
pair0dime, I've seen that research batted around, it helps to tie it right in the with the diagram that says how endothelin-1 is raised by refluxing blood flow. 224% higher - that is a big number and a big clue.
Posted: Thu Apr 14, 2011 1:19 pm
by Brightspot
Thanks for the great post Cece.
Followed the link to the study, but only the first 100 words are avilable unless you pay for it.
Posted: Thu Apr 14, 2011 2:57 pm
by MegansMom
Great thread. And things for the researchers to consider , when trying to figure out the causes of restenosis.
Endothelial health "post-procedure" protocols would be a great idea.
Re: diagram for the effects of reversed blood flow
Posted: Fri Jan 06, 2012 12:43 pm
by Cece
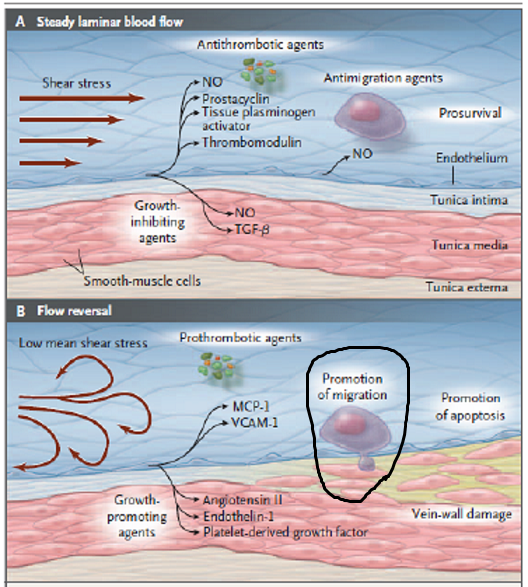
Here's an additional image, so we can understand this in its entirety!
First the shear stress image, and I've circled the part about migration:
Then the second image, from this website:
http://www.mult-sclerosis.org/news/Sep2 ... sease.html
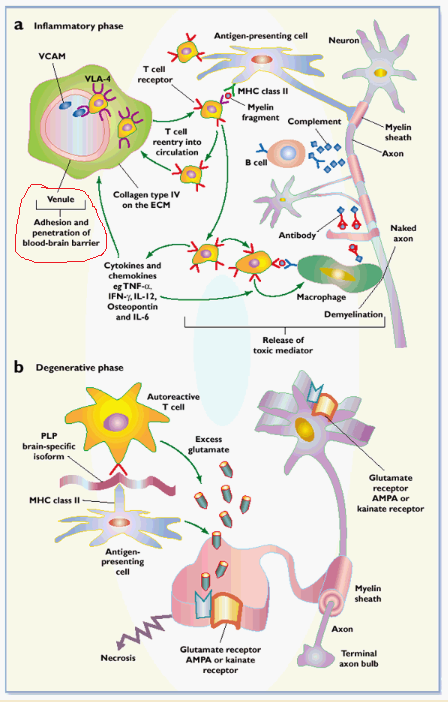
Migration of cells across the endothelium, as circled in the first diagram, means the same as adhesion and penetration of the blood brain barrier, as circled in the second diagram.
The first diagram is showing the effects of low shear stress, as occurs in CCSVI, on the endothelium. The second diagram is showing the difference between the inflammatory component of MS as seen in relapsing-remitting MS, and the noninflammatory degenerative phase seen in primary or secondary progressive MS.