Page 2 of 3
Posted: Tue Apr 05, 2011 1:57 pm
by Nunzio
Liberation wrote:
Where did you have the operation? 14 mm sounds a smaller balloon, doesn't it? Mine was done with a smaller balloon and I got restenoses also in a week or two. My doctor told me that they just started a new group of patients whose veins will be dilated 4 times a year. They think it is a safer way than using extra large balloons. It would be really good if IRs would exchange notes with each other and they would have reliable data on their patients. We would save lot of time, damages and unneccessary procedures.
Did they say anything about why restenoses happens so quickly? I guess it is a pure elastic recoil. Did they dilate the valves or break the annulus?
My last procedure was done by Dr. Sclafani. 14 mm. balloon was used for my first procedure and 16 mm for the last two. Having the procedure 4 times/year wouldn't help me; I would need to repeat it once per week.
Nobody knows why the quick restenosis. It might be elastic recoil, fusion of the valve leaflets or extrinsic compression from a muscle, tendon or blood vessel or a combination of the above.
I think a 16 mm balloon would dilate the valve and stretch the annulus but I do not think it would break it.
Time will tell
Posted: Tue Apr 05, 2011 3:37 pm
by civickiller
Nunzio, did you ever get checked for TOS? Your blockages, if I'm seeing correctly, seems to be right at where bones are.
Posted: Tue Apr 05, 2011 7:26 pm
by drsclafani
Liberation wrote:Nunzio wrote:We have experience of more than 400 patients. We will do what ever is necessary
according to the findings on Angiogram. Cutting, double balloon, balloons with
wire. large balloons up to 23 mm
So it looks to me he is still using the balloons to break the annulus around the valve, not just stretched it.
If my recollection is right, others like dr Sclafani breaks the annulus as well, isn't it? I was asking a well respected vascular surgeon who got the international prize of the American Association of vascular surgeons in 2010 and he was working with dr Zamboni in the past about this. He told me that he does not support the "breaking'" of the "annulus" for many reasons, one of them was that remodelling of the vein can happen. He is the head of the department which carries out CCSVI operations. I have a great respect for him, just like I do for dr Sclafani. For restenosis, and he is sure of it,after one year of follow up it would be pretty high. Restenosis, after one year of follow up is at least 50%. According to him, the mechanism of restenosis is due to the vein wall structure not to differences in technique.
Nunzio and liberation:
i am backing off trying to break the annulus. Now that i understand more fully the nature of the stenosis, i will try avoid it whenever possible. However if the vein is 3-4 millimeters in diameter and i think that the annulus is just too small to allow much blood through it, then i will push a bit harder since there is not much flow as things are . OnPerhaps in the future isurgical resection will be a better alternative. although we would need mo re data to suggest it
Posted: Wed Apr 06, 2011 4:23 am
by Liberation
..........
Posted: Wed Apr 06, 2011 4:24 am
by Liberation
.
Posted: Wed Apr 06, 2011 1:27 pm
by Nunzio
civickiller wrote:Nunzio, did you ever get checked for TOS? Your blockages, if I'm seeing correctly, seems to be right at where bones are.
Yes, I did and TOS was not found; I still could have CTOS or CTNVS as it is called now. In that case a stent or an open sky procedure should help.
http://www.thisisms.com/ftopicp-97920-.html#97920
Posted: Wed Apr 06, 2011 1:28 pm
by Liberation
......
Posted: Wed Apr 06, 2011 5:18 pm
by lucky125
I don't think that we can realistically expect doctors to fully collaborate at this point in time. There are just too many different rationales, and techniques being used.
I saw McGuckin after he treated my friend on Monday. He treated her IJVs, azygos, l. renal, and iliac veins. I know other doctors who would absolutely consider his approach too aggressive at this point, because there are no studies about treating the iliac and renals. Zamboni didn't touch them.
Until each doctor has a robust number of treatments under his belt, and is keeping good data, we will not know who is having the best long term results.
We may not know the intimate details of what they are sharing with each other, and that's o.k. As long as they are talking amongst themselves, even if they are not necessarily agreeing, we are all benefiting.
We are still in the wild, wild West of CCSVI treatment. A very knowledgeable person in this field told me that we won't have a "best practice" model that all doctors will follow for another 5 years.
I didn't wait, and I wouldn't expect anyone else to wait 5 years. But we are very much in a "caveat emptor" time in CCSVI treatment.
Posted: Wed Apr 06, 2011 6:59 pm
by Cece
That's the third report of Dr. McGuckin ballooning renal veins. Either the rest of the IRs are undertreating this vein or he is overtreating (and I don't know which it is right.) How big of a vein is it? Is there precedence in the literature for ballooning the renal vein as there is for the iliac and May Thurner?
I agree with what you've said in regards to wild wild west, no standardization, caveat emptor.
Posted: Wed Apr 06, 2011 9:47 pm
by civickiller
Nunzio wrote:civickiller wrote:Nunzio, did you ever get checked for TOS? Your blockages, if I'm seeing correctly, seems to be right at where bones are.
Yes, I did and TOS was not found; I still could have CTOS or CTNVS as it is called now. In that case a stent or an open sky procedure should help.
http://www.thisisms.com/ftopicp-97920-.html#97920
ive read that upper cervical care can help
Posted: Thu Apr 07, 2011 6:00 am
by Liberation
..........
Posted: Thu Apr 07, 2011 6:48 am
by lucky125
Cece wrote:That's the third report of Dr. McGuckin ballooning renal veins. Either the rest of the IRs are undertreating this vein or he is overtreating (and I don't know which it is right.) How big of a vein is it? Is there precedence in the literature for ballooning the renal vein as there is for the iliac and May Thurner?
I agree with what you've said in regards to wild wild west, no standardization, caveat emptor.
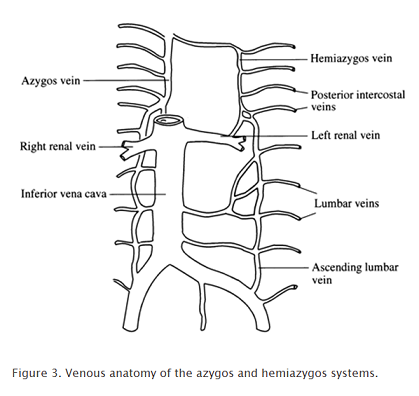
Dr. McGuckin justifies treating the left renal vein because it drains the hemiazygos. There is no studies about treating it that I am aware of.
Just because one doctor is doing it doesn't mean that he is more right than a doctor who does not.
Cece, I guess until you and I go to medical school and become IRs ourselves, we'll never know more than they do! I'm busy this week, so I'll have to put off my applications until at least next week! ;o) Sigh... So many goals, so little time and money!
Maybe I can at least learn to ride a horse and twirl a lasso so I can hang out with them in the Wild West!
Nicole
Posted: Thu Apr 07, 2011 7:32 am
by Cece
lucky125 wrote:Cece, I guess until you and I go to medical school and become IRs ourselves, we'll never know more than they do!
We shall have to set our sights lower and aim for knowing more than our neurologists.


Posted: Thu Apr 07, 2011 8:05 am
by frodo
just for the record maybe we can mention here the operation of Rici, as a possible technique for special cases.
I remember that there was a thread before about "different problems in veins", but I cannot find it. That could be a better place for this information, but maybe this is a good place too.
As far as I have read, the problem for Rici was a abnormally wide IJV with problems for draining. The solution was an open neck surgery in which the vein was sewed and then the extra portion was cut.
There was no need to cut the blood flow during the procedure and the vein was never open.
Posted: Thu Apr 07, 2011 10:37 am
by Liberation
..........