Page 3 of 7
Posted: Wed May 18, 2011 8:22 am
by DrCumming
drsclafani wrote:
mike, i would not be satisfied with those results.i think that there is incomplete opening of the valve as shows by the contrast in the cuffs.
i believe that five atmospheres will NOT be successful. Did you check for elastic recoil? did you repeat IVUs after venoplasty? I suspect that you will see that the valve leaflets are still not completely open.
i am still using high pressure. i havent yet done the calculation, but i am suspecting that pressure in range of 8-23 are necessary to eradicate elastic recoil
Hi Sal, not sure if you read the entire text or I didn't explain well enough.
What we are seeing post ballooning is the entrance of the EJ. In this case the EJ and IJ form a confluence before entering the SCV. If you look at the pre and post IVUS results the area of the IJ just above this confluence is 92 mm2. The post ballooning area at the level of the valve plane is 85 mm2. Very little residual stenosis. Any larger of a balloon would have lead to some dilation of the normal adjacent vein. At 14 mm the area of the balloon is 154 mm2. This is already significantly greater then the normal IJ area of 92 mm2. A 16 mm balloon with an area of 200mm would have been too large in my opinion and would have induced too much intimal damage and subsequent hyperplasia.
I have seen a rash of high grade restenosis and hyperplasia in patients that I have seen in follow up (both my patients and others).
This gets back to the rules of IR.....
It easy to come back and do more and its very hard to undo something you have done.
So the images.... with some better labeling

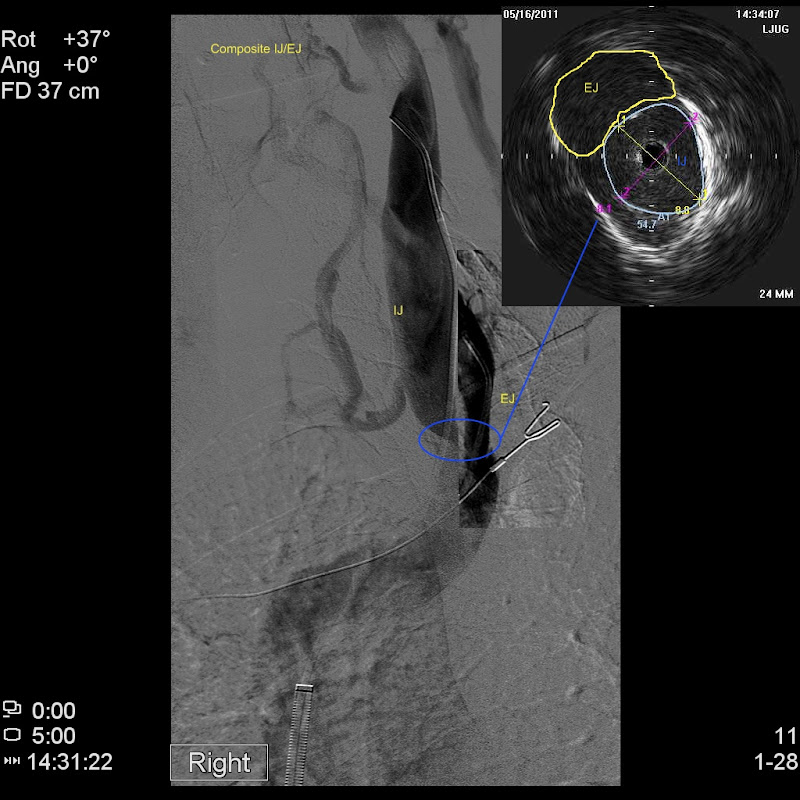
SCV venogram showing the confluence of EJ/IJ

Here is a composite image with venograms of the IJ and EJ superimposed with the IVUS at that level.
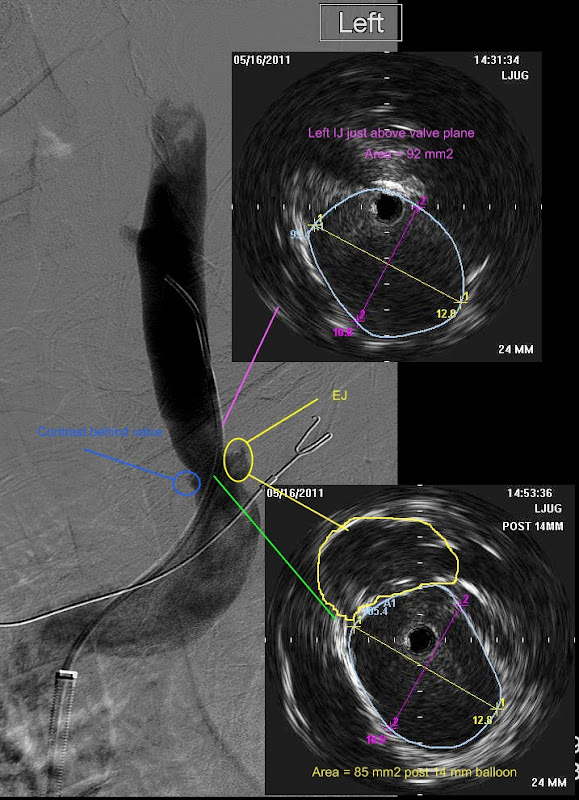
and here is the post ballooning image.
I don't think this is under treated.
Posted: Fri Jul 01, 2011 8:14 pm
by Cece
DrCumming wrote:Cons: I have some ideas to try and speed up procedure times with IVUS - will see how they work out. Cost is cost. If outcomes are better then its worth it.
If you see this, what ideas did you have to speed up procedure times with IVUS? Did they work out?
Pros: Definitely see stenosis not seen on venogram. Better sizing and assessment of venoplasty, with less intimal damage. Does this improve patency/durability - I do not know.
Any closer to knowing if the use of IVUS improves patency or durability?
Posted: Fri Jul 01, 2011 8:23 pm
by Cece
drsclafani wrote:i think that there is incomplete opening of the valve as shows by the contrast in the cuffs.
Does 'contrast in the cuffs' mean when there is what looks like cuffs extending off of the main vein?
I wish we knew who is right about the use of high pressure.

Y'all should have a doctors' thread or something, you know. (It is something to see the back-and-forth on the level that you both deliver.)
Posted: Fri Jul 01, 2011 10:21 pm
by drsclafani
DrCumming wrote:drsclafani wrote:
mike, i would not be satisfied with those results.i think that there is incomplete opening of the valve as shows by the contrast in the cuffs.
i believe that five atmospheres will NOT be successful. Did you check for elastic recoil? did you repeat IVUs after venoplasty? I suspect that you will see that the valve leaflets are still not completely open.
i am still using high pressure. i havent yet done the calculation, but i am suspecting that pressure in range of 8-23 are necessary to eradicate elastic recoil
Hi Sal, not sure if you read the entire text or I didn't explain well enough.
What we are seeing post ballooning is the entrance of the EJ. In this case the EJ and IJ form a confluence before entering the SCV. If you look at the pre and post IVUS results the area of the IJ just above this confluence is 92 mm2. The post ballooning area at the level of the valve plane is 85 mm2. Very little residual stenosis. Any larger of a balloon would have lead to some dilation of the normal adjacent vein. At 14 mm the area of the balloon is 154 mm2. This is already significantly greater then the normal IJ area of 92 mm2. A 16 mm balloon with an area of 200mm would have been too large in my opinion and would have induced too much intimal damage and subsequent hyperplasia.
I have seen a rash of high grade restenosis and hyperplasia in patients that I have seen in follow up (both my patients and others).
This gets back to the rules of IR.....
It easy to come back and do more and its very hard to undo something you have done.
So the images.... with some better labeling
SCV venogram showing the confluence of EJ/IJ
Here is a composite image with venograms of the IJ and EJ superimposed with the IVUS at that level.
and here is the post ballooning image.
I don't think this is under treated.
i cant disagree with you on balloon size, just pressure and i am still not convinced that this contrast that i thought was under the cusp is really that. Admittedly, i am not seeing the entire venogram so i will defer to you.
the external jugular vein is supposed to enter the subclavian vein lateral to this position. Granted, variation in venous anatomy is the name of the game
CV and IVUS = full diagnosis ???
Posted: Sat Jul 02, 2011 10:23 am
by MarkW
Watching developments in diagnosis leads me to conclude that only Catheter Venography (CV) and Intravenous Ultrasound (IVUS) used in combination are the only diagnosis methods to provide a complete diagnosis.
Do you agree or disagree ???
The problem is that there appear to be only 3 centres in the world who are offering CV and IVUS in combination. That makes staying local nearly impossible. Costs are higher if IVUS is a pre-requisite.
Should patients by requesting IVUS from more centres ???
I must declare that I recently travelled to Brooklyn to test my "CV and IVUS is best" conclusion.
MarkW
Re: CV and IVUS = full diagnosis ???
Posted: Sat Jul 02, 2011 10:38 am
by DrCumming
MarkW wrote:Watching developments in diagnosis leads me to conclude that only Catheter Venography (CV) and Intravenous Ultrasound (IVUS) used in combination are the only diagnosis methods to provide a complete diagnosis.
Do you agree or disagree ???
The problem is that there appear to be only 3 centres in the world who are offering CV and IVUS in combination. That makes staying local nearly impossible. Costs are higher if IVUS is a pre-requisite.
Should patients by requesting IVUS from more centres ???
I must declare that I recently travelled to Brooklyn to test my "CV and IVUS is best" conclusion.
MarkW
MarkW,
Yes, I agree. As I mentioned in another thread, I would not do these procedures without IVUS. Otherwise you just do not know what you are treating, what balloon size to use, and what is a reasonable end point to the ballooning. There are others in the US using it. Sal might be able to list them (in fact he may have in another thread).
Posted: Sat Jul 02, 2011 11:59 am
by Cece
In fact, he may have in this very thread!
www.thisisms.com/ftopicp-164667.html#164667
Arizona Heart Institute was a surprise, we don't hear much about them.
I agree too Mark, except I've always stated it as venography plus IVUS in the hands of someone who knows how to use IVUS. It doesn't benefit a patient to be among the first handful of CCSVI patients in which the doctor uses IVUS. There is a learning curve to IVUS in CCSVI on top of the learning curve of CCSVI.
Posted: Mon Jul 04, 2011 5:26 am
by CureOrBust
EHC in the UK re: IVUS. New gold standard? wrote:...diagnosed by Doppler ultrasound with CCSVI. Vic Fernando had found a narrowing in the upper right internal jugular and an abnormal valve on the same side. When the dye was injected into the veins, the blood flow looked normal and there was no sign of any narrowing. My heart sunk, I could not believe that on the very occasion we had this famous surgeon visiting the clinic, the patient had no abnormality !
...
In this case the IVUS completely agreed with the Doppler Ultrasound findings, contradicting the findings of venography.
I understand this question may be a bit much to ask at this early stage, but roughly, or if at all, what percentage chance do you think would there be of someone not showing issues on a standard external Doppler and no issues in a venography, but IVUS would find something? from a purely diagnosis perspective.
Of course this is personal, as I have had two treatments (venographies with each including angioplasty) and a follow up (external) ultrasound, where no issues were found. I still have MS. NB: they did not perform any cranial ultrasound measures, but I didn't have any when it was performed before my treatments.
Posted: Mon Jul 04, 2011 9:40 am
by 1eye
This may not be the right thread to bring this up, but here goes: I was thinking of a possible way to deal with not using opaque dye. As I recalled there was a procedure done with only IVUS because the patient was allergic to the dye. It occurred to me, the balloon can be made visible to x-ray without dye touching the inside of the vein, if the dye is used inside the balloon. The physics of a liquid-filled balloon is different, but may be even better for the application. A liquid is non-compressible, and so the balloon will be more resilient. Rupture can still occur, but I think it is less likely. I think much greater pressures are possible without rupture, although whether they are usable is another story. All this would have to be verified in vitro.
Posted: Tue Jul 05, 2011 8:08 am
by drsclafani
CureOrBust wrote:EHC in the UK re: IVUS. New gold standard? wrote:...diagnosed by Doppler ultrasound with CCSVI. Vic Fernando had found a narrowing in the upper right internal jugular and an abnormal valve on the same side. When the dye was injected into the veins, the blood flow looked normal and there was no sign of any narrowing. My heart sunk, I could not believe that on the very occasion we had this famous surgeon visiting the clinic, the patient had no abnormality !
...
In this case the IVUS completely agreed with the Doppler Ultrasound findings, contradicting the findings of venography.
I understand this question may be a bit much to ask at this early stage, but roughly, or if at all, what percentage chance do you think would there be of someone not showing issues on a standard external Doppler and no issues in a venography, but IVUS would find something? from a purely diagnosis perspective.
Of course this is personal, as I have had two treatments (venographies with each including angioplasty) and a follow up (external) ultrasound, where no issues were found. I still have MS. NB: they did not perform any cranial ultrasound measures, but I didn't have any when it was performed before my treatments.
Perhaps it is just me, but i find that the majority of azygous valvular abnormalities are not visible on venography but visible on IVUS.
But IVUS is not just about making a diagnosis. it is also about a treatment plan, balloon sizes, and assessment of the effects of angioplasty. It can also detect dissections after angioplasty that may go unrecognized without ivus.
s
Posted: Tue Jul 05, 2011 8:12 am
by drsclafani
1eye wrote:This may not be the right thread to bring this up, but here goes: I was thinking of a possible way to deal with not using opaque dye. As I recalled there was a procedure done with only IVUS because the patient was allergic to the dye. It occurred to me, the balloon can be made visible to x-ray without dye touching the inside of the vein, if the dye is used inside the balloon. The physics of a liquid-filled balloon is different, but may be even better for the application. A liquid is non-compressible, and so the balloon will be more resilient. Rupture can still occur, but I think it is less likely. I think much greater pressures are possible without rupture, although whether they are usable is another story. All this would have to be verified in vitro.
1eye
the balloon is always filled with a diluted contrast media solution. Air is rarely used but even that would be visible. You must have a visible balloon to know whether you have stretched open the vein.
in the case you allude to, we used an MRI contrast media instead of iodinated contrast media to reduce risk in the rare situation where balloon rupture could cause a problem.
Posted: Tue Jul 05, 2011 8:45 am
by Cece
drsclafani wrote:Perhaps it is just me, but i find that the majority of azygous valvular abnormalities are not visible on venography but visible on IVUS.
But IVUS is not just about making a diagnosis. it is also about a treatment plan, balloon sizes, and assessment of the effects of angioplasty. It can also detect dissections after angioplasty that may go unrecognized without ivus.
s
Dissections in the vein wall? Have you seen that in a CCSVI patient?
The majority of azygous valvular abnormalities are not visible on venography but visible on IVUS, by your observation! That's pretty big.
Posted: Tue Jul 05, 2011 1:32 pm
by 1eye
the balloon is always filled with a diluted contrast media solution. Air is rarely used but even that would be visible. You must have a visible balloon to know whether you have stretched open the vein.
in the case you allude to, we used an MRI contrast media instead of iodinated contrast media to reduce risk in the rare situation where balloon rupture could cause a problem.
Well, you're thank goodness a long long ways ahead of the likes of me. Air being visible is nothing I would ever have guessed. Sure, why use iodine if there is the remotest chance the balloon breaks and you get anaphylaxis or something. When they put you in charge, they might've gotten it somewhat correct, there. To use the world's most extreme example of understatement.
Posted: Tue Jul 05, 2011 7:14 pm
by drsclafani
1eye wrote:the balloon is always filled with a diluted contrast media solution. Air is rarely used but even that would be visible. You must have a visible balloon to know whether you have stretched open the vein.
in the case you allude to, we used an MRI contrast media instead of iodinated contrast media to reduce risk in the rare situation where balloon rupture could cause a problem.
Well, you're thank goodness a long long ways ahead of the likes of me. Air being visible is nothing I would ever have guessed. Sure, why use iodine if there is the remotest chance the balloon breaks and you get anaphylaxis or something. When they put you in charge, they might've gotten it somewhat correct, there. To use the world's most extreme example of understatement.
who put me in charge?
if they had, i would now be completing my safety and feasibility trial, funded, of course, by big pharma, who, by the way, would have invested in ivus and high pressure balloons. the randomized trial would include montel, you and a few of my friends and me, a few neurologists and the CEO of two major ballooon manufacturers as controls. It would have started on july 4th and be completed on thanksgiving.
just in time for a nice christmas present

Posted: Wed Jul 06, 2011 1:14 am
by CureOrBust
drsclafani wrote:CureOrBust wrote:EHC in the UK re: IVUS. New gold standard? wrote:...diagnosed by Doppler ultrasound with CCSVI. Vic Fernando had found a narrowing in the upper right internal jugular and an abnormal valve on the same side. When the dye was injected into the veins, the blood flow looked normal and there was no sign of any narrowing. My heart sunk, I could not believe that on the very occasion we had this famous surgeon visiting the clinic, the patient had no abnormality !
...
In this case the IVUS completely agreed with the Doppler Ultrasound findings, contradicting the findings of venography.
I understand this question may be a bit much to ask at this early stage, but roughly, or if at all, what percentage chance do you think would there be of someone not showing issues on a standard external Doppler and no issues in a venography, but IVUS would find something? from a purely diagnosis perspective.
Perhaps it is just me, but i find that the majority of azygous valvular abnormalities are not visible on venography but visible on IVUS.
But IVUS is not just about making a diagnosis. it is also about a treatment plan, balloon sizes, and assessment of the effects of angioplasty. It can also detect dissections after angioplasty that may go unrecognized without ivus.
I was obviously not clear enopugh, my question was if these issues were not visible under fluoroscope, would they present themselves as flow issue under a standard CCSVI doppler; errr... by standard I guess we would have to take Zamboni's measures...