Page 5 of 7
Posted: Wed Aug 31, 2011 1:00 pm
by Vivianne766
Cece wrote:
My crazy thought is, taking this further, if a patient is up and about while the veins are still healing, would it help to occasionally hold one's breath? The rationale would be that this would increase the blood in the jugulars and get those sticky walls away from each other, at least for the time being. I've seen how it looks on IVUS when the vein expands.
I think about that too... !
Posted: Wed Aug 31, 2011 7:23 pm
by HappyPoet
DrCumming wrote:Sure would love to have a percutaneous valulotome.
Here's a link to a TIMS' thread about Dr. Zamboni's device for percutaneous valve leaflet cutting and removal and valve replacement (using bovine tissue and a stent):
Ultimate CCSVI treatment for defective valves of IJV
DrCumming wrote:2 tries at venoplastly. Any other options then a stent for round 3?
Because you mentioned it, if I was this patient, I would want to discuss the pros and cons of waiting to see if a percutaneous valvulotome might become available.
Unintended consequences
Posted: Thu Sep 01, 2011 12:27 am
by MarkW
Hello Dr T.
Pleased by your comments. Unintended consequences of postings and writing is enormous on the internet. Prof Zamboni wrote about liberating bloodflow (years ago) and a whole LIBERATION industry has grown up. As a business analyst I suggest that this has delayed CCSVI therapy by several years. Canadians still cannot get CCSVI therapy but often demand liberation, a connection probably.
MarkW
Size is not the only question
Posted: Thu Sep 01, 2011 12:46 am
by MarkW
I realise that women reading my post will have heard the male comment: " size does not matter".
But here are my questions for a full picture of the therapy you are using:
- What pressure (atmospheres) do you use in the balloon ?
- What duration (seconds) of inflation do you use ?
- How many repetitions of inflation do you use ?
- In a stenosed valve which dimension do you use to estimate balloon size ?
- Do you over stretch valves ? What percentage ? Or just stretch to 100% of 'normal' size.
I realise there is not just one answer but pwMS need guidance on the therapy they are seeking.
For me unless my diagnosis included both IVUS and catheter venogram it was not a full diagnosis (it did). Do you agree ??
MarkW
Posted: Fri Sep 02, 2011 12:03 pm
by DrCumming
Hi Mark,
Great questions. I do agree with your statement about needing to us both IVUS and venography. They are complimentary tools.
Sizing is critical. The IJ does not like to be over dilated. I think that significant balloon over sizing and cutting wires/balloons are in general not a good idea.
How to do the sizing is difficult. In virginal veins, the narrowing is almost always valve related. So, I look at this region of the vein with IVUS. We can see the opening of the valve and the area of the underlying normal vein at this location. I also look carefully at the vein above and below the valve plane. I typically start with a balloon equal or slightly larger in size to the normal surrounding vein. I try to never inflate > 10 ATM unless I know I am definitely only dilating the valve. I then repeat the IVUS and retreat with a larger balloon if needed. End point is to open the valves to at least the size of the surrounding normal vein and better to have them completely open to the size of the vein at the level of the valves (note: this area is often a fair bit larger then the normal surrounding vein so that always trying to achieve this means a balloon too big for the surrounding vein and causing too much intimal injury).
The majority of restenosis I see is not from recurrent valve leaflets (except the last case I posted) but from narrowed vein with intimal hyperplasia and scarring. This is occurring from too aggressive venoplasties.
I am not sure repeated inflations or long inflations make any difference. I no longer do them.
I have really enjoyed reading your posts. Its great that so many people with different backgrounds are looking at this.
End point???
Posted: Wed Oct 12, 2011 1:01 pm
by DrCumming
Case 6: 55 yo female with PPMS since 2005. Images from the right IJ.
Discussion is around what is a reasonable end point and inflation pressure.
Initial venogram showing typical stenosis at the level of the valve.

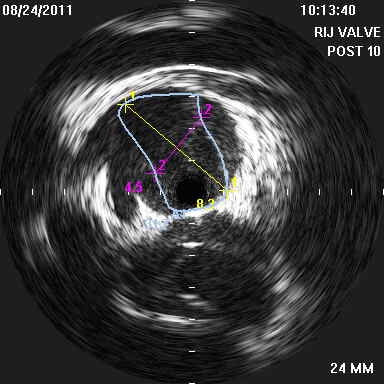
IVUS at valve

Area of valves is 29 mm2 and the normal jugular is 49 mm2.
IVUS Post 10 mm balloon, waist resolved at 5 ATM. Still residual stenosis. Do we stop or continue at this point???
We decided to continue with dilation with a 12 mm balloon. Waist in balloon needed 18 ATM to resolve.
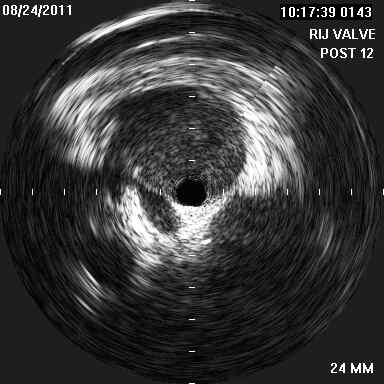
Post IVUS looks great with no residual valve leaflets or narrowing
Post 12 mm venogram also looks great.

Patient placed on Pradaxa. Follow up US at 6 weeks shows complete occlusion of the right IJ.

In this case, we had an excellent venographic and IVUS outcomes but ended up with an occluded vein.
So, was the residual stenosis with 10mm ok? Should this have been the end point? Or with the 12mm balloon should we have stopped at a lower pressure? When limiting balloon pressure to 10 ATM or less I have not seen any occlusions like this. Yet, I have also dilated many veins with > 20 ATM and had good outcome but more occlusions as well.
Re: End point???
Posted: Wed Oct 12, 2011 3:57 pm
by Cece
Patient placed on Pradaxa. Follow up US at 6 weeks shows complete occlusion of the right IJ.
I hate occlusions.
I'll check your numbers against Dr. Sclafani's handy balloon sizing chart....
http://www.thisisms.com/forum/chronic-c ... ml#p178072
A CSA of 49 would be ballooned with a 9 mm balloon, with the possibility of going up to 10 mm if resistant. So maybe the 12 mm balloon was too big.
I will guess the endpoint should have been a 10 mm balloon with an ATM less than 18 but greater than 5.
I am no IR, so take this guess for what it's worth.
Re: End point???
Posted: Wed Oct 12, 2011 4:08 pm
by DrCumming
Cece wrote:Patient placed on Pradaxa. Follow up US at 6 weeks shows complete occlusion of the right IJ.
I hate occlusions.
I'll check your numbers against Dr. Sclafani's handy balloon sizing chart....
http://www.thisisms.com/forum/chronic-c ... ml#p178072
A CSA of 49 would be ballooned with a 9 mm balloon, with the possibility of going up to 10 mm if resistant. So maybe the 12 mm balloon was too big.
I will guess the endpoint should have been a 10 mm balloon with an ATM less than 18 but greater than 5.
I am no IR, so take this guess for what it's worth.

well, I know if I had left it, and the patient didn't improve, then Sal would have chastised me for undertreating the patient.

agree, 10 mm was the right starting size. and with the 10 mm balloon we had easy inflation to profile, but residual narrowing on repeat ivus.
part of the problem with this patient (and others I have seen) is that there was a high (C1) narrowing limiting flow in this vein.
many factors too consider.
Re: IVUS
Posted: Thu Oct 13, 2011 1:27 pm
by MarkW
Interesting to view IVUS in combination with venograms.....................MarkW
Re: End point???
Posted: Thu Oct 13, 2011 2:19 pm
by Cece
DrCumming wrote:part of the problem with this patient (and others I have seen) is that there was a high (C1) narrowing limiting flow in this vein.
And this limited flow could contribute to a higher risk of thrombosis?
The other question might be if the endpoint should be earlier with a PPMS patient, if PPMS is seeing less benefit from CCSVI treatment, then less should be risked. I don't yet know if it is true if PPMS sees less benefit.
A previous theory has been that complications are more common in the LIJV, but this one occurred in the RIJV. I'd assume this was the smaller of the two jugulars. But why does smaller size lead to more complications, if it does?
I note that you prescribed Pradaxa, but it did not prevent this occlusion. I have not yet heard much about outcomes on Pradaxa. It sounds like it should be a good anticoagulant.
Any plans to attempt to get through the occlusion? Did the patient have any improvements that were subsequently lost?
I don't think we have good answers for what to do in cases of residual narrowing. I believe this is similar to what was seen (residual narrowing) in my own left jugular in my July procedure. There was a possibility of stopping after the 10 mm balloon, but the choice was made to go to a 12 mm balloon.
It is good that there is no active doctors' thread, or I wouldn't get to weigh in like this, but it is unfortunate that there is no active doctors' thread. We also miss out on any thoughts the other doctors might have on Dr. Sclafani's cases.
Re: End point???
Posted: Sat Oct 15, 2011 6:42 pm
by drsclafani
DrCumming wrote:Cece wrote:Patient placed on Pradaxa. Follow up US at 6 weeks shows complete occlusion of the right IJ.
I hate occlusions.
I'll check your numbers against Dr. Sclafani's handy balloon sizing chart....
http://www.thisisms.com/forum/chronic-c ... ml#p178072
A CSA of 49 would be ballooned with a 9 mm balloon, with the possibility of going up to 10 mm if resistant. So maybe the 12 mm balloon was too big.
I will guess the endpoint should have been a 10 mm balloon with an ATM less than 18 but greater than 5.
I am no IR, so take this guess for what it's worth.
well, I know if I had left it, and the patient didn't improve, then Sal would have chastised me for undertreating the patient.
agree, 10 mm was the right starting size. and with the 10 mm balloon we had easy inflation to profile, but residual narrowing on repeat ivus.
part of the problem with this patient (and others I have seen) is that there was a high (C1) narrowing limiting flow in this vein.
many factors too consider.
mike
as if anyone really cares about my critiques. I have had all the complications i care to have in the beginning of my work. In the past six months, the only thromboses were two patients who stopped taking anticoagulation. Makes me wonder about the risks in those patients who are given no anticoagulation or just aspirin.
i am curious: in addition to the pradaxa, did you give an antiplatelet medication. I give both.
my general rule is i will increase size of balloon between 25-75% of size of the normal vein. 12 mm would have been over 100% increase. My experience, like your current one is that the vein cannot tolerate that much stress.
how long after the treatment did you discover the thrombosis? did you attempt to salvage?
Re: End point???
Posted: Sat Oct 15, 2011 6:46 pm
by drsclafani
DrCumming wrote:
In this case, we had an excellent venographic and IVUS outcomes but ended up with an occluded vein.
So, was the residual stenosis with 10mm ok? Should this have been the end point? Or with the 12mm balloon should we have stopped at a lower pressure? When limiting balloon pressure to 10 ATM or less I have not seen any occlusions like this. Yet, I have also dilated many veins with > 20 ATM and had good outcome but more occlusions as well.
mike, i dont think it is the pressure that is the problem. it is using high pressures with a balloon too large. I average 13 ATM in the last 150 cases.
Re: IVUS
Posted: Sun Oct 16, 2011 1:36 pm
by Cece

Am I seeing correctly that this is the lumen of the occluded jugular? I added arrows.
Re: End point???
Posted: Sun Oct 16, 2011 2:33 pm
by DrCumming
drsclafani wrote:
mike
as if anyone really cares about my critiques. I have had all the complications i care to have in the beginning of my work. In the past six months, the only thromboses were two patients who stopped taking anticoagulation. Makes me wonder about the risks in those patients who are given no anticoagulation or just aspirin.
i am curious: in addition to the pradaxa, did you give an antiplatelet medication. I give both.
my general rule is i will increase size of balloon between 25-75% of size of the normal vein. 12 mm would have been over 100% increase. My experience, like your current one is that the vein cannot tolerate that much stress.
how long after the treatment did you discover the thrombosis? did you attempt to salvage?
sal,
without critiquing, there will be no learning.
when speaking about sizing, are we using area or diameter? i think we should stick to area measurements.
i hope we can stimulate discussion about what are appropriate end points for the procedure.
here is what i typically do....
size the IJ immediately distal (above) the valve plane. i do not believe we can change the size of this segment vein, so there is no point making the valves open more than this. this is the inflow. size at the valves - both the maximum opening of the valves and the area of the normal vein.
first ballooning is done using a balloon with an area about 10-20% greater than the vein immediately above the valves or the vein at the valve (which ever is smaller). in this case we did not have a 9mm balloon available and so we started at 10. we could have started at 8mm.
the question is what to do after the 10mm balloon with ivus still showing poorly opening leaflets. i can see a few options.
1. do nothing
2. repeat dilation with 10mm balloon
3. dilate with a cutting balloon
4. go bigger (we do not have an 11 mm balloon, so 12 was our next option).
since the waist in the balloon resolved at 5 atm, i don't think 2 or 3 would have offered anything.
so that leaves us with 1 or 4.
this will be great discussion for the workshop
Re: End point???
Posted: Sun Oct 16, 2011 2:36 pm
by DrCumming
drsclafani wrote:DrCumming wrote:
In this case, we had an excellent venographic and IVUS outcomes but ended up with an occluded vein.
So, was the residual stenosis with 10mm ok? Should this have been the end point? Or with the 12mm balloon should we have stopped at a lower pressure? When limiting balloon pressure to 10 ATM or less I have not seen any occlusions like this. Yet, I have also dilated many veins with > 20 ATM and had good outcome but more occlusions as well.
mike, i dont think it is the pressure that is the problem. it is using high pressures with a balloon too large. I average 13 ATM in the last 150 cases.
yes, this was a combination of too much pressure and too large of a balloon.
i typically have been limiting pressure to less than 6 atm. this case was the first time in probably 3 months of going over 15 atm.