Use of high-pressure balloons in CCSVI by Dr. Jan de Letter
Posted: Thu Oct 20, 2011 3:43 pm
http://www.ccsvi-online.com/news/studie ... ment-ccsvi
Dr. Jan de Letter of Bruges compares and contrasts the use of normal balloons, cutting balloons, and high pressure balloons in CCSVI. He also provides images of a ballooning done at 14 atm. (In the wall tension thread, I was discussing placement of the balloon, and in Dr. de Letter's images, you can see what it looks like when the balloon is centered on the stenosis instead of lower down.)
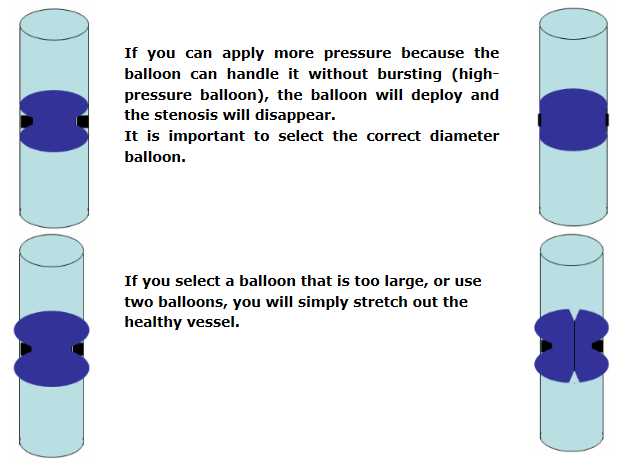
I like the one on the top right, where the stenosis gives way. The lower two images should both result in a higher dilating force on the stenosis, so the stenosis may yet give way, but at least in the one with the larger balloon, the wall definitely gets more dilating force against it too.
This next part is good:
Dr. Jan de Letter of Bruges compares and contrasts the use of normal balloons, cutting balloons, and high pressure balloons in CCSVI. He also provides images of a ballooning done at 14 atm. (In the wall tension thread, I was discussing placement of the balloon, and in Dr. de Letter's images, you can see what it looks like when the balloon is centered on the stenosis instead of lower down.)
Does the use of the "kissing balloons" methods with two balloons used to increase pressure result in stretching of the healthy vein wall when compared to high pressure balloons? I thought it only resulted in a larger insertion scar down at the groin. But here is the image:Techniques used for arteries cannot simply be transferred to veins. Flow rate and pressure in arteries are much higher. Furthermore, artery walls have a completely different structure than vein walls. Experiences with dialysis patients - where a vein is connected directly to an artery in a small surgical procedure - show that classic balloons used in arteries cannot apply the pressure required to open stenoses that develop in these veins (so-called dialysis fistulas). These veins are too stiff due to connective tissue bands. The use of balloons with a larger diameter than the vessel or the use of two balloons also does not offer a solution. This only results in stretching the healthy wall to either end of the stenosis, which is obviously not the objective.
To solve this conundrum, two different techniques were chosen, the previously mentioned cutting balloon being the first. By inflating this balloon multiple times, turning it a little each time, the desired effect is achieved. The disadvantage of this technique is that local bleeding may occur, as the blades can cut through the thinner vein wall. The other solution is to use high-pressure balloons. The effects are the same as for arteriosclerosis, however high-pressure balloons can be inflated to 16 bars without the risk of the balloon tearing. This allows far more force to be applied to the stenosis, and sufficiently stretches out the connective tissue that causes the narrowing. Tests have shown that the use of stents in dialysis fistulas affect the inner lining of the vein in the long term, resulting in new stenosis and even complete occlusions.
I like the one on the top right, where the stenosis gives way. The lower two images should both result in a higher dilating force on the stenosis, so the stenosis may yet give way, but at least in the one with the larger balloon, the wall definitely gets more dilating force against it too.
This next part is good:
He goes on to take aim at other doctors' methods, which are cutting balloons and the use of two balloons at once to increase pressure, as being more aggressive and certain to lead to vein damage. He also does not recommend the use of stents in CCSVI given the experience with dialysis fistulas.For over a year now, I have been using high-pressure balloons to dilate the parts of veins where stuck valves, membranes and band-shaped thickenings are causing problems. Using high-pressure balloons, I have treated hundreds of patients with good and lasting results. It is important to note I see practically no re-stenoses (new narrowing) in patients in the long term. My conclusion is that the connective tissue strands in the band-shaped stenosis are sufficiently broken up, and no damage has been done to the wall of the treated vein.