Page 1 of 1
etiology of CCSVI
Posted: Fri Feb 01, 2013 10:45 am
by Cece
http://www.unboundmedicine.com/medline/ ... rocephalus
Unbound MEDLINE
Increased intracranial volume: a clue to the etiology of idiopathic normal-pressure hydrocephalus?
Abstract
BACKGROUND AND PURPOSE
The etiology of idiopathic normal-pressure hydrocephalus (NPH) is unknown. The purpose of this study was to examine the hypothesis that NPH begins in infancy as benign external hydrocephalus due to decreased uptake of CSF by the arachnoid villi. Since this occurs before the sutures fuse, a secondary hypothesis is that the intracranial volumes of patients with NPH should be larger than those of healthy individuals.
METHODS
Intracranial volumes of 51 patients with clinically suspected NPH were compared with those of age- and sex-matched control subjects. All patients underwent phase-contrast CSF velocity MR imaging. They had aqueductal CSF stroke volumes of at least 60 microL, which was 50% higher than previously published normal values. Intracranial volumes were measured and compared between groups.
RESULTS
The average intracranial volume for men with NPH (n = 22) was 1682 mL compared with 1565 for male control subjects (n = 55). The NPH volume averaged 118 mL (7.5%) larger than the control volume (P = .003). The average intracranial volume for women with NPH (n = 29) was 1493 mL compared with 1405 mL for female control subjects (n = 55). The NPH volume was 88 mL (6.3%) larger than the control volume (P = .002).
CONCLUSION
Patients with NPH have intracranial volumes significantly larger than normal, suggesting that the initial insult occurs before the sutures fuse at 1 year of age. The patients somehow remain asymptomatic until their later years, when a second insult must occur, leading to symptomatic NPH.
This could be a way to investigate the etiology of CCSVI. It depends on if people with CCSVI have decreased uptake of cerebral spinal fluid by the arachnoid villi in the sinuses which drain into the jugulars which are blocked. If so, then wouldn't the same increase in intracranial volume be seen in pwMS as is seen in people with NPH? This would also require the CCSVI to be prior at birth due to congenital malformation. Sutures fuse at 1 year old so the expansion happens before then. If there is increase in intracranial volume, would that affect measurements of brain atrophy?
Re: etiology of CCSVI
Posted: Fri Feb 01, 2013 1:02 pm
by Anonymoose
Oh good...a new lead! I'm not even going to try to wrap my head around this CSF concept. I have faith that you can do it though.
Why couldn't the "first insult" happen after the sutures fuse? Couldn't pwms have NPH w/o large intercranial volume?
Now I've got to look up the arachnoid villi...
Re: etiology of CCSVI
Posted: Fri Feb 01, 2013 1:19 pm
by Cece

there's a picture here:
http://radiographics.rsna.org/content/2 ... nsion.html
Little bumps in the venous sinuses through which cerebrospinal fluid drains.
and an ivus image of an arachnoid granulation:
http://www.thisisms.com/forum/chronic-c ... ml#p167713
If you get your head around the CSF information, share it with me, because my understanding of CSF is still rudimentary.
Re: etiology of CCSVI
Posted: Fri Feb 01, 2013 1:30 pm
by Anonymoose
Ha! I'm not even going to try...I'm going to dabble. When you have prepared a presentation suitable to explain CSF to the Sesame Street audience, I will be sitting criss-cross-applesauce in the front row.
10 seconds later....
Oh no! Read this!
http://www.ncbi.nlm.nih.gov/books/NBK27998/
There is evidence that absorption of CSF by the arachnoid villi occurs by a valve-like process, permitting the one-way flow of CSF from the subarachnoid spaces into the venous sinuses. CSF absorption does not occur until CSF pressure exceeds the pressure within the sinuses. Once this threshold is reached, the rate of absorption is proportional to the difference between CSF and sinus pressures. A normal human can absorb CSF at a rate up to six times the normal rate of CSF formation with only a moderate increase in intracranial pressure.
I will not make up a theory about this...I will not make up a theory about this...
Re: etiology of CCSVI
Posted: Fri Feb 01, 2013 1:53 pm
by Anonymoose
This can't make me make up another theory either...even though I could see SF building pressure around the cranial nerves....
http://www.ncbi.nlm.nih.gov/books/NBK27998/ (same link)
Cerebrospinal fluid circulates through the ventricles, over the surface of the brain, and is absorbed at the arachnoid villi and at the cranial and spinal nerve root sheaths
Re: etiology of CCSVI
Posted: Sat Feb 02, 2013 4:08 pm
by Anonymoose
If the arachnoid villi aren't draining sufficiently due to increased pressure in the venous sinuses, does that mean more CSF is being pushed through the cranial and spinal nerve roots because the absorption at those points isn't pressure dependent? If so, maybe the autonomic dysfunction is caused by more than just pressure issues. Maybe the increased CSF flow through the nerve roots causes local inflammation which dies down over time after PTA causing improvements beyond those experienced on the table.
The incurable theorist

Re: etiology of CCSVI
Posted: Sat Feb 02, 2013 5:15 pm
by Cece
Nothing wrong with being a theorist.
Do you think the CCSVI researchers are going to figure all of this out? And how long will it take? Some of the questions can't be answered without neurologists involved in the research.
Re: etiology of CCSVI
Posted: Sun Feb 03, 2013 3:02 am
by MarkW
Cece wrote:Nothing wrong with being a theorist. Do you think the CCSVI researchers are going to figure all of this out? And how long will it take? Some of the questions can't be answered without neurologists involved in the research.
Hello Cece,
I have a suspicion that the CCSVI researchers are looking in the wrong place, just like the Neuros. The widely expressed view is that CCSVI is congenital. But CCSVI is generally detected later than at birth. My theory is that MS and CCSVI are epigenetic diseases. This means we (PwMS/CCSVI) have the genetic code to develop MS and CCSVI present at birth but something in the environment (or not in the environment) changes this genetic code later in life. Some research is being published about this:
Lancet Neurol. 2013 Feb;12(2):195-206. doi: 10.1016/S1474-4422(12)70309-5.
Epigenetic mechanisms in multiple sclerosis: implications for pathogenesis and treatment.
Huynh JL, Casaccia P.
Source
Department of Neuroscience, Mount Sinai School of Medicine, New York, NY, USA; Department of Genetics and Genomic Sciences, Mount Sinai School of Medicine, New York, NY, USA.
Abstract
Clinical neurologists and scientists who study multiple sclerosis face open questions regarding the integration of epidemiological data with genome-wide association studies and clinical management of patients. It is becoming evident that the interplay of environmental influences and individual genetic susceptibility modulates disease presentation and therapeutic responsiveness. The molecular mechanisms through which environmental signals are translated into changes in gene expression include DNA methylation, post-translational modification of nucleosomal histones, and non-coding RNAs. These mechanisms are regulated by families of specialised enzymes that are tissue selective and cell-type specific. A model of multiple sclerosis pathogenesis should integrate underlying risk related to genetic susceptibility with cell-type specific epigenetic changes occurring in the immune system and in the brain in response to ageing and environmental stimuli.
Copyright © 2013 Elsevier Ltd. All rights reserved.
PMID: 23332363 [PubMed - in process]
The answer is decades away for CCSVI. This is why I advocate treating symptoms (CCSVI, Vit D3 etc) rather than waiting for probably inconclusive research.
Kind regards,
MarkW
Spelling corrected
Re: etiology of CCSVI
Posted: Sun Feb 03, 2013 6:33 am
by Anonymoose
Cece wrote:Nothing wrong with being a theorist.
Do you think the CCSVI researchers are going to figure all of this out? And how long will it take? Some of the questions can't be answered without neurologists involved in the research.
Don't they have a neurologist involved already? I do think they are going to figure it out and I think it will be soon (3 years max?). The beauty of PTA for CCSVI is that it is just a change in hemodynamics. There are a limited number of resulting changes that could cause improvement...and even fewer changes that could cause the on the table improvements. They just need to play whack-a-mole with the possibilities and then be really loud about their findings because I don't get the sense neurologists pay much attention to anything MS unless it's a DMD.
Maybe we could build a float for the New Years parade...a translucent model of the brain with some jugulars hanging down...a clown or two squeezing them to block flow...some girls in braids and lederhosen pumping a keg of CSF into the ventricles...ooo...and some hot italian guys prying the clowns off the jugulars. That might get their attention. Why stop there? We could build CCSVI land! Some of those collateral veins would make for a mean roller coaster...
I think I should go eat breakfast now.
Re: etiology of CCSVI
Posted: Sun Feb 03, 2013 1:12 pm
by Cece
CCSVI land, lol!
Anonymoose wrote:Don't they have a neurologist involved already?
Dr. Zamboni works with Dr. Salvi, a neurologist. Dr. Zivadinov at the University of Buffalo is the most prominent neurologist researching CCSVI. Dr. Hubbard in California is a neurologist. There is a neurologist, whose name slips me, who may partner with Dr. Dake on his long-anticipated CCSVI trial. Dr. Fox at the Cleveland Clinic is a neurologist who contributed to the CCSVI field with his name added to Claude Diaconu's paper finding CCSVI malformations in autopsied MS patients. So I can count on one hand the number of neurologists involved in CCSVI.
The widely expressed view is that CCSVI is congenital. But CCSVI is generally detected later than at birth. My theory is that MS and CCSVI are epigenetic diseases. This means we (PwMS/CCSVI) have the genetic code to develop MS and CCSVI present at birth but something in the environment (or not in the environment) changes this genetic code later in life.
I'm comfortable with the idea of both congenital CCSVI and acquired CCSVI.
Anything in the body that can go wrong, does go wrong, at least for somebody.
Re: etiology of CCSVI
Posted: Sun Feb 03, 2013 2:08 pm
by vesta
Interesting when last summer ("A Plausible CCSVI Origin Theory" July 17 ) I first suggested that CCSVI could be "developmental" which would account for the epidemiological factors, my idea was generally dismissed. It's congenital, period. Well, no, maybe not. I'll reprint my opening statement, though I would now change it slightly since valve abnormalities seem the major factor. Why has Japan seen a major increase in MS at an ever younger age over the past 30 years? Change in genes, or maybe diet? Why do women between puberty and menopause have a greater incidence of MS? Genes? Why complicate what might be quite simple, if deadly.
Also see "Five CCSVI MS Types" Dec 16, 2012 which opened the CSF subject.
"Multiple Sclerosis blood vessels "deformed" by childhood
stress cannot accommodate the blood flow. I believe the auto-immune activity is secondary to the true cause of MS, blood refluxes which injure the brain and spinal cord. The origin of the refluxes may be structural 1) CCSVI stenosis (as proposed by Professor Zamboni) and/or cerebrospinal fluid pressure or 2) it may be a stress reaction to toxic substances.
Let's re-think first causes. And then move on to real solutions.
Epidemiological studies on MS show that those who grow up close to the equator have less chance to develop MS than those living in latitudes closer to the poles. It is the latitude where one lives before age 15 that counts, not where one lives subsequently. It is therefore thought that the lack of sunlight – hence Vit D – is a factor in susceptibility to MS. Vit D is recommended for M.S. patients.
But perhaps a better explanation of the geographical factor is Winter Cold.
The shoulders and neck typically tense up under stress thus restricting circulation to and from the brain. Cold weather stiffens the muscles. Winters bring the body aches of colds and flus. Illness itself (e.g. Clamydia pneumoniae, Mononucleosis, Guillaume Barré) may damage the cell walls and valves of the vascular system.
It is also said that MS patients tend to be high powered, ambitious people. Tensed up in other words. MS cases cluster in northern Europe and North Amerca. Let’s say growing up in a culturally demanding family environment (or in any case stressful) while subject to Cold weather and frequent colds and flus actually compresses and deforms the circulatory system in the child’s developing body.By the time he/she reaches age 15, the stunted blood vessels can no longer accommodate the blood flow. MS first appears in adolescents, seldom in children. Let’s compare the deformity to ancient Chinese footbinding where the tiny child’s foot cannot support the adult woman.
Food intolerances, especially to wheat and dairy products, can further compound the stress. The Neolithic agricultural revolution dates back not much more than 10,000 years, a blink of the eye in terms of biological evolution. Bowel problems are a sure sign of food “stress”. The significant increase in MS cases in Japan over the past 30 years points to food toxicity as root cause.
And the disadvantage of being female. Between puberty and menopause at least two-thirds of MS patients are women. This implies that gynecological problems (including menstrual cramps and birth control pills) both stress and require "poisoning" treatment which impact negatively the vascular system. Perhaps monthly menstrual cramps in a growing girl actually "stunt" the circulatory system. Perhaps female hormones affect the vascular system negatively. Factors of Stress.
Maybe the real story behind MS is the damage to the blood vessels caused by growing up female in a 1) driven, ambitious or otherwise stressful family environment compounded by 2) a climate of Cold winters which contribute to 3) frequent viral illnesses compounded by 4) an intolerance to the wheat and lactose of a Neolithic diet."
MS Cure Enigmas.net
Re: etiology of CCSVI
Posted: Thu Feb 07, 2013 7:15 am
by Anonymoose
Cece,
You already have the Sesame Street version of csf flow on tims. I should have known.
http://www.thisisms.com/forum/chronic-c ... 18752.html
Great explanation. Thanks!
Re: etiology of CCSVI
Posted: Thu Feb 07, 2013 8:49 am
by Cece

But do you see this quote from that link?
The latter was pretty but not intuitively understandable to me...
That was me trying to admit that I don't understand CSF flow!!
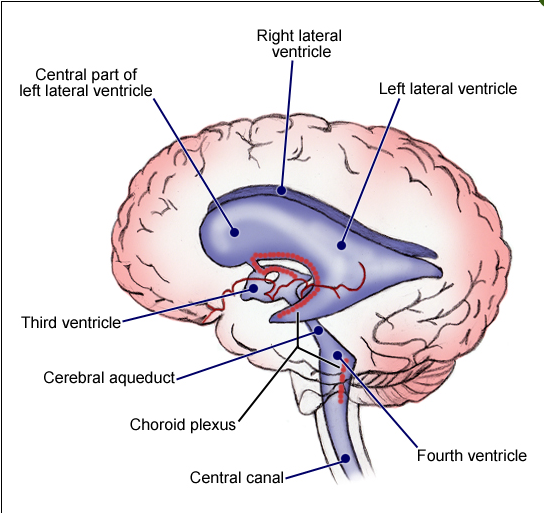
Step 1: Choroid plexus in the lateral ventricles produces CSF.
Ok, but what is a choroid plexus again? How and why does it produce CSF?
 http://emedicine.medscape.com/article/1923254-overview
http://emedicine.medscape.com/article/1923254-overview
I'm not sure I'm ready for Step 2 yet but ok moving on
Step 2: CSF flows through interventricular foramina into third ventricle.
Third ventricle is enlarged in MS.
Step 3: Choroid plexus in the third ventricle adds more CSF.
Now the choroid plexus is in third ventricle too? Choroid plexus gets around.
Step 4: CSF flows down cerebral aqueduct to fourth ventricle.
"cerebral aqueduct" is in the image above
Step 5: Choroid plexus in the fourth ventricle adds more CSF.
Step 6: CSF flows out two lateral apertures and one medial aperture.
Step 7: CSF fills subarachnoid space and bathes external surfaces of brain and spinal cord.
Step 8: At arachnoid villi, CSF if reabsorbed into venous blood of dural venous sinuses.
The bathing of the brain and spinal cord is its main task. Reabsorption is into the dural sinuses, which drain into the jugulars.