Page 2 of 3
Posted: Fri Jun 26, 2009 7:07 am
by mrhodes40
OK now this is just getting crazy.......
FROM HERE
Pathophysiology of cervical myelopathy.
Baptiste DC, Fehlings MG.
Division of Cell and Molecular Biology, Toronto Western Research Institute and Krembil Neuroscience Centre, Toronto Western Hospital, University Health Network, University of Toronto, Toronto, Ontario, Canada.
BACKGROUND CONTENT: Cervical myelopathy is a group of closely related disorders usually caused by spondylosis or by ossification of the posterior longitudinal ligament and is characterized by compression of the cervical spinal cord or nerve roots by varying degrees and number of levels. The decrease in diameter of the vertebral canal secondary to disc degeneration and osteophytic spurs compresses the spinal cord and nerve roots at one or several levels, producing direct damage and often secondary ischemic changes. PURPOSE: Clinicians who treat cervical myelopathy cord injuries should have a basic understanding of the pathophysiology and the processes that are initiated after the spinal cord has been injured. STUDY DESIGN/SETTING: Literature review. METHODS: Literature review of human cervical myelopathy and clinically relevant animal models to further our understanding of the pathological mechanisms involved. RESULTS: The pathophysiology of cervical myelopathy involves static factors, which result in acquired or developmental stenosis of the cervical canal and dynamic factors, which involve repetitive injury to the cervical cord. These mechanical factors in turn result in direct injury to neurons and glia as well as a secondary cascade of events including ischemia, excitotoxicity, and apoptosis; a pathobiology similar to that occurring in traumatic spinal cord injury. CONCLUSIONS: This review summarizes some of the significant pathophysiological processes involved in cervical myelopathy.
The dynamic factors that result in repetitive injury to the cord in the CCSVI model would be the reflux and ongoing changes in the venous pressure. Note that these result in direct injury to the glia and neurons as well as ischemia (lack of blood flow) excitotoxicity and apoptosis. ... These are all things that are discussed in MS lesions as well.
Taken with the white matter grey matter stuff from earlier in the thread....man!
Posted: Fri Jun 26, 2009 7:49 am
by mrhodes40
Now this is just getting plain wierd
HERE
Jugular venous reflux in cerebral radionuclide angiography: an explanation.
Bok B, Marsault C, Aubin ML, Bar D, Aboulker J.
A case of isotopic jugular venous reflux, reaching the opposite jugular vein, is described. Phlebography and aortography were simultaneously performed in this patient and showed the innominate vein narrowed and pinched between the sternal notch and the aortic arch. This narrowing depends on the position of the left arm
\
SO this person was fine until they moved their left arm and when they did it caused reflux because the innominate vein ran into the aortic arch and plugged it up.
Take this in association with the other papers that talk about jugulars beig OK to take out---UNLESS there is a flow disturbance and excess flow. What if this anomaly of arm pinch is something some people have and in combination with jugular stenosis it results in a PERIODIC reflux situation?
How about if you were painting with your arms up for hours or something like that?
relapse?
speculation! But can you imagine how hard it would be to suss out all of these kind of unusual factors like this? Thank goodness the consistent thing is the stenosis.
Re: Myelopathy associated with bilateral jugular vein...
Posted: Sun Jun 28, 2009 10:48 am
by cheerleader
NHE wrote:Holy myelopathies Batman 

The following text is from one of my MRI reports that was done 2 years after I was initially diagnosed. The above reference makes me wonder if there's a connection in my own case?

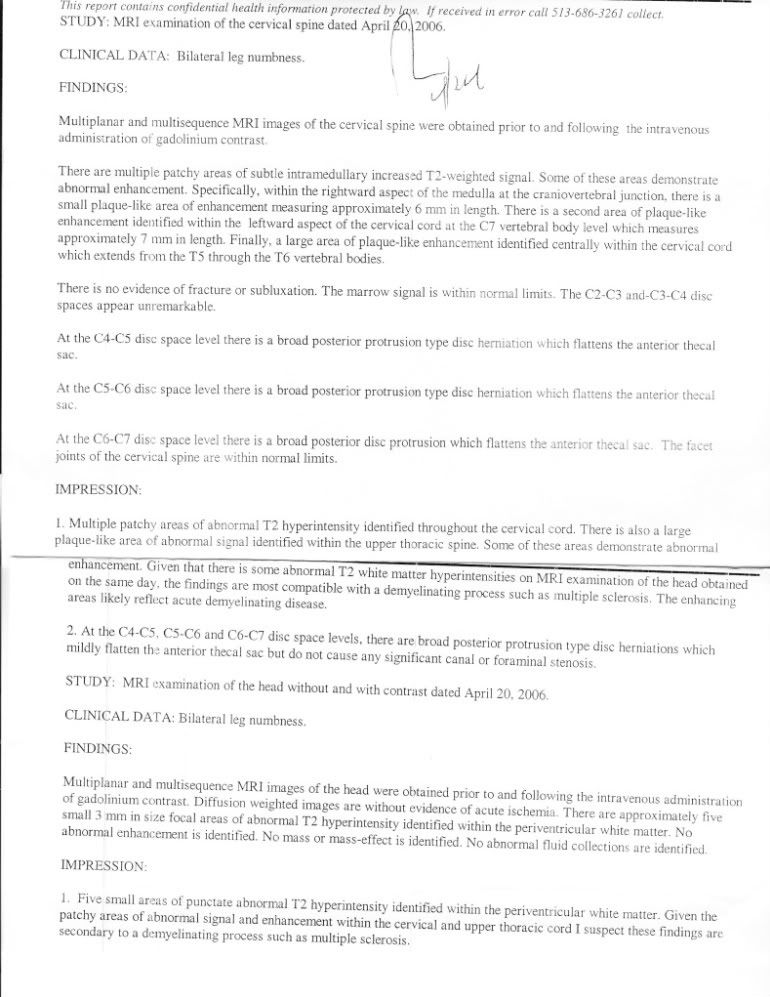
Impression:
MR imaging of the cervical spinal cord demonstrates only minimally increased T2 signal intensity within the spinal cord at the C6-C7 disc space level, the site of the prominent diffuse disc bulge. Findings are less prominent than on the prior examination. Imaging of the cervical spinal cord is otherwise unremarkable.
MR Cervical Spine.
Technique: Sagittal and axial T1 and T2 images were obtained of the cervical spine with and without contrast.
Findings: There is straightening of the cervical lordotic curvature. At the C6-C7 level there is a broad-based, disc bulge which causes anterior extradural indentation of the thecal sac without compete effacement of CSF anterior to the spinal cord. There is not a focal disc herniation.
There is mild narrowing of the neural foramen, bilaterally. There is no alteration in spinal cord contour. There is minimally increased T2 signal intensity within the spinal cord posterior to the inferior aspect of C6 and the superior aspect of C7 which is distinctly less prominent than on the prior examination.
Spinal cord at other levels is normal. There are no structural alterations of the foramen magnum.
In any case, at least on the surface, the MRI report seems to be consistent with the CCSVI hypothesis.

It looks like the pieces of the puzzle are starting to fit together or maybe I'm just looking at it with CCSVI colored glasses.

Comments on this are of course welcome as always.
NHE
NHE...
It is interesting, isn't it? Jeff had a similar note on his MRI report about disc bulging, but no herniation (unrelated to his MS-the doc said, probably aging) at C3-4. Jeff also had a lesion in that area. After seeing his venography, and the occlusion of his jugular vein and collateral veins at that exact location, it made a bit more sense. Most MSers have cervical spine issues, most MSers are showing jugular blockage. The jugs and the cervical spine share some real estate.
cheer
Posted: Sun Jun 28, 2009 11:05 am
by skydog
The jugs and the cervical spine share some real estate. This is something I will be talking over with Dr. Dake. I have a very pronounced offset in the vertebrae from a skiing fall at 18 yrs old and have been dealing with back issues ever since. I will also be asking for his thoughts on my use of the inversion table that has greatly reduced the offset in my spine. Actually I have gained back 3/8 of a inch in height. Hopefully there is also more space available for both the jugs and cervical spine to share. Trapped inside by the heat !!! Mark
Posted: Sun Jun 28, 2009 12:03 pm
by Terry
Here is mine. I almost could have just copied yours, NHE.
So maybe this is an effect of the CCSVI, not the cause of it, right?
This is stretching the page, but I don't know how to fix it. Help?
Posted: Sun Jun 28, 2009 12:40 pm
by cheerleader
Hey Terry...
Wow. Another cervical spine situation. Yeah, we're thinking this is the effect of CCSVI. If we look at the disease model of myelopathy created by tortuous/stenosied veins, then we can infer that the blocked jugulars create reflux and allow those collateral veins to form and leak along the cervical spine. The veins come first in that model. yikes... I really wanna see how Jeff's cervical spine is looking, if there's any difference.
cheer
Posted: Sun Jun 28, 2009 6:50 pm
by Terry
I need help with this. To me, as I read, it looks like the herniated discs are causing the probems. You all are seeing that the CCSVI is the cause, Please, can someone explain all this to me?
Thank you in advance.
Terry
Posted: Tue Jun 30, 2009 3:19 pm
by mrhodes40
Hey terry glad I can add to this... you have good eye it is the discs but:
The paper I posted showed that the cases they showed had neuropathy but it was not the DISC itself that was pressing on the nerve....
It was the disc pressing on the VEINS.....and the veins got so swollen THEY pressed on the nerves!!!!
So on MRI they could see that the disc was out and it was NOT pressing the nerve so it looked good but the veins themselves were the thing pressing and that was shown in a venogram.
wild huh?
My friend Island Girl has terrible neck issues and discs out but not pressing the nerves it seems on MRI. She is very anxious to see what they see with regards to her MRV
Posted: Wed Jul 01, 2009 1:33 pm
by ladystewart
To all!!
I am out of wait!! and wish to try CCSVI ASAP. I read all and am constantly viewing!!
I will tell my age because I was diagnosed at 35(42 now) and have not had MS for even 8 years yet. I am about to get a wheelchair. I am relapsing progressive and will be SPMS. My hands are getting crazy from typing![/i][/u]
Posted: Wed Jul 01, 2009 2:10 pm
by Loobie
Sounds great lady!! From another 42 year old who got dx'd at 35.
Posted: Wed Jul 01, 2009 3:52 pm
by mrhodes40
Gosh Lady Stewart can you call Dr. Dake? See what is in there?
Posted: Wed Jul 01, 2009 4:24 pm
by ladystewart
I called and my doctor(Neuro-) office is faxng info. I talked to Alex and she will have Dr. Dake view!! I will keep all posted.
Posted: Thu Jul 02, 2009 3:28 am
by Loobie
Man that's some good news!!
Posted: Wed Aug 05, 2009 11:34 am
by wyleone76
Hello to everyone, I am new to this board as you probably all know...I stumbled upon it while googling last night. I have one quick question and more to follow most likely . Is it that increased intracranial pressure can in some cases cause brain lesions? Is that correct? If anyone or cheerleader if you can clarify that for me I would be so happy! ifquote="cheerleader"]
zap wrote:But is this myelopathy comparable to that seen in MS lesions?
As I understood this case study, high pressure in the veins that run inside the vertebrae had them engorged and crowding, even crushing, the spinal cord in the space they shared. (Cervical Spondylotic Myelopathy)
Then when the drainage was allowed to flow through the jugulars instead, the internal veins slimmed down and the decompressed cord could heal.
Terrific point...zap. The collateral veins that formed on this patient put pressure on the spine- the mechanism of demyelination is not exactly the same, but engorged veins also leak and can damage tissue. The main point I wanted to make about this study is that we will hear from doctors that the IJVs are not essential for drainage, that the vertebral and collateral veins can take the load just fine. What these doctors are saying is that is not true. Without jugular drainage, collateral veins will leak, or become engorged and put pressure on surrounding tissue and bone.
What my husband and this patient share is this:
bilateral jugular stenosis from the base of the skull to the jaw
cervical spinal myelopathy (both created by collateral veins)
Increased intracranial pressure
-but they have 2 different diagnosis...because my husband's intracranial hypertension created lesions in his brain, and got him diagnosed with MS. These doctors knew the patient's history with venous issues, so they looked to her jugulars first. And the mechanism for healing is the same...get rid of the engorged collateral veins and let the jugs do their job, and myelopathy can heal.
make sense?
cheer[/quote]



Posted: Wed Aug 05, 2009 12:10 pm
by cheerleader
wyleone76 wrote:Hello to everyone, I am new to this board as you probably all know...I stumbled upon it while googling last night. I have one quick question and more to follow most likely . Is it that increased intracranial pressure can in some cases cause brain lesions? Is that correct? If anyone or cheerleader if you can clarify that for me I would be so happy!
Welcome, Wyleone...if you're new here, we recommend reading the two "stickies" at the top of the forum, as well as these forums:
http://www.thisisms.com/ftopict-6488.html
http://www.thisisms.com/ftopict-7374.html
It's alot to digest, but hopefully this information will answer more of your questions.
The mechanism of lesion formation that Dr. Zamboni proposes is put forward in his paper "The Big Idea" in the research sticky. He likens it to iron deposition found in chronic venous lesions in the legs. In this case, a stressed endothelial layer of blood vessels leaks iron and other plasma particles into the brain and spine, activating the immune system and causing lesions. We've also been discussing how this reflux caused by CCSVI can also create slowed perfusion, intracranial pressure and hypoxia (a lack of oxygen) in the brain and spine. All of these features have been researched and found in the MS brain....and CCSVI explains the method for this injury.
Keep reading, and ask away. We're all learning together.
cheer