Hi MRI report result stated few small foci of non enhancing t2/ flair signal involving the right frontal white matter are noted, particularly along the right superior frontal gyrus, nonspecific and possibly incidental with differential considerations including sequelae of prior infectious/ inflammatory process and demyelinating disease.
Everything else was normal . Symptoms are just ptosis or drooping of the right eyelid. Nothing else
If someone can please decipher the terminology and language and let me know what this means
I appreciate the help
Thank you
MRI report
Re: MRI report
Did you ask your doctor?

Re: MRI report
I'm not an MRI expert, but I'll offer what I can.mrna wrote:Hi MRI report result stated few small foci of non enhancing t2/ flair signal involving the right frontal white matter are noted, particularly along the right superior frontal gyrus, nonspecific and possibly incidental with differential considerations including sequelae of prior infectious/ inflammatory process and demyelinating disease.
Everything else was normal . Symptoms are just ptosis or drooping of the right eyelid. Nothing else
If someone can please decipher the terminology and language and let me know what this means
...non enhancing: means that they're old lesions and not sites of active inflammation.
...flair signal: This is a special MRI mode that removes the water signal to improve resolution.
FLAIR MRI = Fluid-Attenuated Inversion Recovery MRI
https://radiopaedia.org/articles/fluid- ... n-recovery
...right superior frontal gyrus: "The superior frontal gyrus is a broad longitudinal gyral formation running in an anteroposterior direction along the dorsal-medial margin of the frontal lobe until the precentral sulcus. That part of this gyrus on convex surface is distinguished as lateral SFG. It is bounded by the longitudinal fissure and the superior frontal sulcus."
http://www.thehumanbrain.info/brain/sections.php
...nonspecific and possibly incidental with differential considerations including sequelae of prior infectious/ inflammatory process and demyelinating disease: The lesion could be due to a variety of factors and is not specific to MS. Possible reasons given include prior infection or inflammation. Many things can cause lesions in the brain, e.g., migraines, sleep apnea, etc.
Here are some examples of MS lesions, many of which are periventricular.
https://radiopaedia.org/search?q=multip ... cope=cases
Re: MRI report
Thank you very much. That was very helpful. Thank you
-
centenarian100
- Family Elder
- Posts: 504
- Joined: Mon Apr 15, 2013 9:51 am
Re: MRI report
to MRNA:
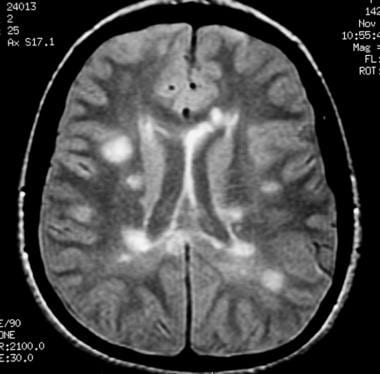
Radiologists often read films in a broad way because they do no know the clinical history of the patient. Many people have non-specific benign white matter lesions that are insignificant. These are common in people as they get older, but they can also be seen in young people, especially those with migraines. For instance, the lesions shown in this MRI are completely benign and insignificant (despite the dubious label posted by a clueless blogger)

Multiple sclerosis usually is associated with lesions which are large, well-demarcated, and in specific anatomic locations such as the corpus callosum, periventricular area, juxtacortical area, and brainstem
You just need a reasonably experienced doctor who will look at your scans and take into account your clinical history and exam and tell you whether the lesions are benign or significant.
Hope this helps
-Cent
Radiologists often read films in a broad way because they do no know the clinical history of the patient. Many people have non-specific benign white matter lesions that are insignificant. These are common in people as they get older, but they can also be seen in young people, especially those with migraines. For instance, the lesions shown in this MRI are completely benign and insignificant (despite the dubious label posted by a clueless blogger)
Multiple sclerosis usually is associated with lesions which are large, well-demarcated, and in specific anatomic locations such as the corpus callosum, periventricular area, juxtacortical area, and brainstem
You just need a reasonably experienced doctor who will look at your scans and take into account your clinical history and exam and tell you whether the lesions are benign or significant.
Hope this helps
-Cent
-
1eye

- Family Elder
- Posts: 3780
- Joined: Wed Mar 17, 2010 3:00 pm
- Location: Kanata, Ontario, Canada
- Contact:
Re: MRI report
You might want to read the thread in the CCSVI forum on the Central Vein Sign. An experienced radiologist can recognize the pattern of lesions as the Cenral Vein Sign, which is usually considered to be consistent witn MS.
This unit of entertainment not brought to you by FREMULON.
Not a doctor.
"I'm still here, how 'bout that? I may have lost my lunchbox, but I'm still here." John Cowan Hartford (December 30, 1937 – June 4, 2001)
Not a doctor.
"I'm still here, how 'bout that? I may have lost my lunchbox, but I'm still here." John Cowan Hartford (December 30, 1937 – June 4, 2001)
-
1eye
- Family Elder
- Posts: 3780
- Joined: Wed Mar 17, 2010 3:00 pm
- Location: Kanata, Ontario, Canada
- Contact:
Re: MRI report
.Multiple sclerosis usually is associated with lesions which are large, well-demarcated, and in specific anatomic locations such as the corpus callosum, periventricular area, juxtacortical area, and brainstem
This, and the MRI accompanying it, is misleading. MS lesions are not necessarily large at all, especially at first, and maybe not ever. The Central Vein Sign will be present even when the lesions are still small. None of mine were anywhere near as large when I was diagnosed. They were very small focal hyperintensities. No contrast was required for my diagnosis. I would definitely consult your radiologist, not this forum.
This unit of entertainment not brought to you by FREMULON.
Not a doctor.
"I'm still here, how 'bout that? I may have lost my lunchbox, but I'm still here." John Cowan Hartford (December 30, 1937 – June 4, 2001)
Not a doctor.
"I'm still here, how 'bout that? I may have lost my lunchbox, but I'm still here." John Cowan Hartford (December 30, 1937 – June 4, 2001)
-
1eye
- Family Elder
- Posts: 3780
- Joined: Wed Mar 17, 2010 3:00 pm
- Location: Kanata, Ontario, Canada
- Contact:
Re: MRI report
You might also want to read to the end of http://www.thisisms.com/forum/chronic-c ... 29390.html where I describe my experience with doctors who order MRIs. You should probably ask for a copy of the radiology report.
This unit of entertainment not brought to you by FREMULON.
Not a doctor.
"I'm still here, how 'bout that? I may have lost my lunchbox, but I'm still here." John Cowan Hartford (December 30, 1937 – June 4, 2001)
Not a doctor.
"I'm still here, how 'bout that? I may have lost my lunchbox, but I'm still here." John Cowan Hartford (December 30, 1937 – June 4, 2001)
-
1eye
- Family Elder
- Posts: 3780
- Joined: Wed Mar 17, 2010 3:00 pm
- Location: Kanata, Ontario, Canada
- Contact:
Re: MRI report
This means we are finally free of these "phenotypes" which are merely ways for insurance people to exclude patients from treatment (on actuarial/financial grounds). Perhaps we can start treating the disease, now that we can identify it.The venocentric distribution of lesions exists in all MS clinical phenotypes (RRMS, SPMS and PPMS)
This unit of entertainment not brought to you by FREMULON.
Not a doctor.
"I'm still here, how 'bout that? I may have lost my lunchbox, but I'm still here." John Cowan Hartford (December 30, 1937 – June 4, 2001)
Not a doctor.
"I'm still here, how 'bout that? I may have lost my lunchbox, but I'm still here." John Cowan Hartford (December 30, 1937 – June 4, 2001)