Thekla wrote: If 'head' related improvements are most common, are there any other approaches to take with lower limb mobility?
i don't want to answer for Dr S but i could offer an opinion.
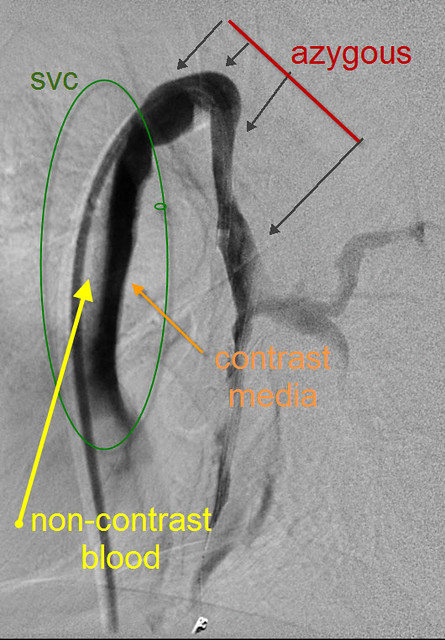
in my "not a doctor" mind, CCSVI is very simple. it means pooling of the blood around the neck area (i know there are lower limb CCSVI too). the heart pumps and blood tries to exit the head/spine region and return to the heart. all of it can't escape because of CCSVI and some pools around the neck and brain area.
if my partner puts her head under water and opens her eyes then her vision is cloudy, she is disoriented. to me that is what CCSVI is like.
lift her head out of the water and look how bright the colors are and how sharp her vision is. that is what treatment for CCSVI is like.
i also believe CCSVI and the resulting pooling of blood is some how related to the damge that doctors label as MS. in some people that damage attacks the nerves that control the lower limbs resulting in mobility issues.
sad as it is, lifing my partner's head out of the water will not fix the MS damage instantly.
the hope is that a healthy brain will be able to repair the damage or relearn around the damage.
i wish i could jump ahead and report any progress. my partner is about to start rehab to see if she can learn to walk without issues again. the signs are all there that she can but MS has had its way for 20 plus years and the road to recovery will be long and hard to travel.