
Hello Darren,
I was having a chat with another patient of Amir's last week whilst sat in the waiting room. She was going through the same thought process.
Actually she'd been to See Dr S earlier this year and is now seeing Amir, she felt with hindsight, like us that she'd probably do the two things the other way around. Get the skeleton sorted, then if you still have issues maybe go the CCSVI route.
I was lying on bed the other night and it was then that it struck me how the two different procedures were dealing with completely separate symptoms.
I know Amir reads this thread and absorbs the vast amount of information that Dr S writes to see if it can in some way help him with what he does. I figured I may as well ask Dr S for his thoughts too.
DrSclafani answers some questions
Re: DrSclafani answers some questions
vesta wrote:
Again, to make a long story short, Dr. Zamboni has discovered the problem – venous blood reflux or CCSVI – but not the sole solution. Detoxification and nutritional therapy coupled with circulation therapies and/or skeletal adjustments may suffice without taking the risk of angioplasty.
Amir wrote Dec 17 2012
I think your final paragraph is apt.
I just want to add that Atlas asymmetry is very dependent on dental symmetry. The later cannot be resolved with a quick adjustment. It needs prolonged treatment.
The former (Atlas) soon goes out of balance if the later is not corrected.
Correcting the later (dental asymmetry) often obviates the correction of the Atlas as demonstrated in a number of our patients.
Thank you for making an excellent contribution.
Vesta -
I believe Dr. Zamboni has discovered the problem – venous blood reflux or CCSVI – but not the sole solution. Detoxification and nutritional therapy coupled with circulation therapies and/or skeletal adjustments may suffice to cure or control MS without taking the risk of angioplasty.
I've concluded there are 5 basic MS types, all of which leading to a reflux of venous blood into the Central Nervous System.
1) CONGENITAL vein malformations. 2) DEVELOPMENTAL vein malformations. 3) AGING vein malformations 4) SKELETAL – Cerebrospinal fluid pressure. 5) TOXIC MS.
As for the current categories of Relapse/Remit and the various Progressive MS's, I don't believe these properly describe the problem and certainly don't point to a solution. The various immunosuppressive drugs developed since 1990 are used only for the Relapse/Remit phase, so once you've hit the Progressive stage, you might as well listen to alternative ideas.
CONGENITAL: This idea is favoured by Phlebologists and Dr. Sclafani. However, it doesn’t account for the epidemiological variations in geography, culture or gender. It certainly can’t explain the dramatic increase in Japanese MS cases over the past 30 years. However, obviously it can be one factor.
DEVELOPMENTAL: My beginning hypothesis was that stress (of many potential origins) damages the veins in the child's developing body so that once adult the veins can no longer accommodate the blood flow. Defects in the circulatory system impede if not outright block blood flow leading from the brain and spinal cord leading to MS "attacks" and subsequent paralysis. It is for this reason that MS first generally manifests during or after adolescence. Dr. Zamboni himself observed deformities in the veins in the back and neck of MS patients. These areas correspond to Acupuncture meridians which control blood/fluid circulation.
AGING MS: The third type develops with age. There is no reason why veins shouldn't harden and malfunction as a part of the aging process. When the valves in veins draining the central nervous system malfunction, blood backs up to injure the myelin sheath.
THE ANGIOPLASTY CURE has been suggested for these types of MS (Congenital, Developmental, Aging) characterized by varied vein malformations - stenosed (narrowed), twisted, exhibiting stuck or deformed valves, or just plain missing. The Italian phlebologist Dr. Zamboni launched the theory he named CCSVI. The treatment consists of threading a catheter through the affected vein and opening it with a “balloon” . Initially the Internal Jugular Veins, the Vertebral Veins and the Chest Azygos vein were treated. Other veins leading from the spinal cord are now treated as well. Development of the Intravenous Ultrasound has allowed Interventional Radiologists to see what is going on inside the vein, determine the appropriate size of the balloon to open the stenosed vein without scarring, and avoid various complications. Stents have been inserted into veins which collapsed after being opened. (Dr. Sclafani believes the early 50% failure rate in the Jugular vein angioplasty occurred because the balloons were too small to open the veins sufficiently.) However, if the balloon is too large it risks scarring the vein lining tissue (endothelium) which might lead to thrombosis – the vein being closed off entirely. There have been cases where, after the initial “liberation”, the vein closes off again and each subsequent intervention leads to more scarring and tissue damage. Some have experienced little if any improvement. (Not all the veins leading from the spinal cord are treated.) Some have found themselves in a worse condition after the angioplasty than before. (One woman reported that her veins shriveled up into useless dried out structures through which no blood could flow.) Risks include brain hemorrhage, blood clots, and stent migration into the heart. Presumably with experience and the development of new techniques and material the few early tragedies which have occurred can be avoided. (Already use of the IntravenousUltrasound has decreased the risk factor dramatically.)
Some have reported dramatic recoveries, often with stents inserted, at least 2 years after Angioplasty. They have been CURED. (I don’t know the longest post operative success story. Treatments began sometime in 2009.) The lives of some have been so transformed that they now wonder if they should declare themselves free of MS and therefore ineligible for disability benefits.
Nonetheless, while some have been apparently cured, the risks of angioplasty are real. Before rushing into the operating theater, consider first treatment of Types 4) SKELETAL and 5) TOXIC MS.
SKELETAL MS: A misaligned skeletal, bone or dental structure can actually restrict the free flow of cerebrospinal fluid which in turn can compress or impede venous blood circulation. Structural problems can be either congenital or developmental in origin (e.g. accidents.) Recent scientific studies have focused on the interdependent dynamic of brain "fluids", the blood and the cerebrospinal fluid (CBF) which bathes the Central Nervous System. Excess cerebrospinal fluid can actually "compress" or limit blood circulation, hence the interest of Chiropractors in adjusting the Atlas bone to assure proper CBF circulation. If the problem is SKELETAL, angioplasty would not be appropriate. In this case it is not a problem INSIDE the vein but OUTSIDE. Chiropractic, Osteopathic or Dental adjustment may suffice to release the brain fluids flow leading to CURE or CONTROL.
FINALLY THERE IS TOXIC MS.
I include in this category not only known toxins such as mercury in dental amalgams, aspartame, glutens and various food intolerances, but myriad microbes/viruses such as mononucleosis, epstein barr, chlamydia, lyme as well as various metabolic disorders such as toxic "gut" and diabetes. OK that's a big category. One might say I am being simplistic. BUT MAYBE IT IS JUST THAT SIMPLE. Whatever stresses the body in those individuals with a compromised vascular system may trigger the blood reflux into the CNS. Illness in childhood may damage the vascular system, stress including toxic stress may trigger the reflux. Toxicity itself may damage the veins. All these factors may stress the vascular system leading to a venous blood reflux. Detoxification, intestinal cleansing, and appropriate nutrition will reduce pressure on the vascular system as well as nurture the brain and heal nerve damage.
CURE: Some MS patients recover through diet cleansing and nutritional therapy alone. Some may have a "temporary" stress reaction to a toxic substance such as aspartame (or mercury in dental almagam fillings.) The reaction is "temporary" in the sense that once the toxin is removed, the MS symptoms disappear. I have even heard that removing glutens from the diet is sufficient to heal.
CONTROL: Dr. Terry Wahls (see You Tube Minding Your Mitochondria) presents another excellent example. She began her treatment by de-toxifying from the MS drugs which were poisoning her and then optimized her nutrition. Her recovery implies that her veins were not actually blocked, but tensed up enough to cause a reflux. Also, she stimulated her blood circulation by electrical stimulation of the bands of muscles on her back, in other words, the bladder meridian. Optimal Diet/Supplements serve two purposes. 1) to prevent stress on the vascular system which might lead to blood reflux and 2) heal damaged tissue.
In addition to nutritional therapy, most MS patients probably will require treatment to enhance blood circulation to prevent blood refluxes – massage, ayervedic massage, acupuncture, self acupressure, osteopathy, chiropractic, swimming.
Again, to make a long story short, Dr. Zamboni has discovered the problem – venous blood reflux or CCSVI – but not the sole solution. Detoxification and nutritional therapy coupled with circulation therapies and/or skeletal adjustments may suffice without taking the risk of angioplasty.
MS Cure Enigmas.net
Post subject: Re: Five CCSVI MS Types
Again, to make a long story short, Dr. Zamboni has discovered the problem – venous blood reflux or CCSVI – but not the sole solution. Detoxification and nutritional therapy coupled with circulation therapies and/or skeletal adjustments may suffice without taking the risk of angioplasty.
Amir wrote Dec 17 2012
I think your final paragraph is apt.
I just want to add that Atlas asymmetry is very dependent on dental symmetry. The later cannot be resolved with a quick adjustment. It needs prolonged treatment.
The former (Atlas) soon goes out of balance if the later is not corrected.
Correcting the later (dental asymmetry) often obviates the correction of the Atlas as demonstrated in a number of our patients.
Thank you for making an excellent contribution.
Vesta -
I believe Dr. Zamboni has discovered the problem – venous blood reflux or CCSVI – but not the sole solution. Detoxification and nutritional therapy coupled with circulation therapies and/or skeletal adjustments may suffice to cure or control MS without taking the risk of angioplasty.
I've concluded there are 5 basic MS types, all of which leading to a reflux of venous blood into the Central Nervous System.
1) CONGENITAL vein malformations. 2) DEVELOPMENTAL vein malformations. 3) AGING vein malformations 4) SKELETAL – Cerebrospinal fluid pressure. 5) TOXIC MS.
As for the current categories of Relapse/Remit and the various Progressive MS's, I don't believe these properly describe the problem and certainly don't point to a solution. The various immunosuppressive drugs developed since 1990 are used only for the Relapse/Remit phase, so once you've hit the Progressive stage, you might as well listen to alternative ideas.
CONGENITAL: This idea is favoured by Phlebologists and Dr. Sclafani. However, it doesn’t account for the epidemiological variations in geography, culture or gender. It certainly can’t explain the dramatic increase in Japanese MS cases over the past 30 years. However, obviously it can be one factor.
DEVELOPMENTAL: My beginning hypothesis was that stress (of many potential origins) damages the veins in the child's developing body so that once adult the veins can no longer accommodate the blood flow. Defects in the circulatory system impede if not outright block blood flow leading from the brain and spinal cord leading to MS "attacks" and subsequent paralysis. It is for this reason that MS first generally manifests during or after adolescence. Dr. Zamboni himself observed deformities in the veins in the back and neck of MS patients. These areas correspond to Acupuncture meridians which control blood/fluid circulation.
AGING MS: The third type develops with age. There is no reason why veins shouldn't harden and malfunction as a part of the aging process. When the valves in veins draining the central nervous system malfunction, blood backs up to injure the myelin sheath.
THE ANGIOPLASTY CURE has been suggested for these types of MS (Congenital, Developmental, Aging) characterized by varied vein malformations - stenosed (narrowed), twisted, exhibiting stuck or deformed valves, or just plain missing. The Italian phlebologist Dr. Zamboni launched the theory he named CCSVI. The treatment consists of threading a catheter through the affected vein and opening it with a “balloon” . Initially the Internal Jugular Veins, the Vertebral Veins and the Chest Azygos vein were treated. Other veins leading from the spinal cord are now treated as well. Development of the Intravenous Ultrasound has allowed Interventional Radiologists to see what is going on inside the vein, determine the appropriate size of the balloon to open the stenosed vein without scarring, and avoid various complications. Stents have been inserted into veins which collapsed after being opened. (Dr. Sclafani believes the early 50% failure rate in the Jugular vein angioplasty occurred because the balloons were too small to open the veins sufficiently.) However, if the balloon is too large it risks scarring the vein lining tissue (endothelium) which might lead to thrombosis – the vein being closed off entirely. There have been cases where, after the initial “liberation”, the vein closes off again and each subsequent intervention leads to more scarring and tissue damage. Some have experienced little if any improvement. (Not all the veins leading from the spinal cord are treated.) Some have found themselves in a worse condition after the angioplasty than before. (One woman reported that her veins shriveled up into useless dried out structures through which no blood could flow.) Risks include brain hemorrhage, blood clots, and stent migration into the heart. Presumably with experience and the development of new techniques and material the few early tragedies which have occurred can be avoided. (Already use of the IntravenousUltrasound has decreased the risk factor dramatically.)
Some have reported dramatic recoveries, often with stents inserted, at least 2 years after Angioplasty. They have been CURED. (I don’t know the longest post operative success story. Treatments began sometime in 2009.) The lives of some have been so transformed that they now wonder if they should declare themselves free of MS and therefore ineligible for disability benefits.
Nonetheless, while some have been apparently cured, the risks of angioplasty are real. Before rushing into the operating theater, consider first treatment of Types 4) SKELETAL and 5) TOXIC MS.
SKELETAL MS: A misaligned skeletal, bone or dental structure can actually restrict the free flow of cerebrospinal fluid which in turn can compress or impede venous blood circulation. Structural problems can be either congenital or developmental in origin (e.g. accidents.) Recent scientific studies have focused on the interdependent dynamic of brain "fluids", the blood and the cerebrospinal fluid (CBF) which bathes the Central Nervous System. Excess cerebrospinal fluid can actually "compress" or limit blood circulation, hence the interest of Chiropractors in adjusting the Atlas bone to assure proper CBF circulation. If the problem is SKELETAL, angioplasty would not be appropriate. In this case it is not a problem INSIDE the vein but OUTSIDE. Chiropractic, Osteopathic or Dental adjustment may suffice to release the brain fluids flow leading to CURE or CONTROL.
FINALLY THERE IS TOXIC MS.
I include in this category not only known toxins such as mercury in dental amalgams, aspartame, glutens and various food intolerances, but myriad microbes/viruses such as mononucleosis, epstein barr, chlamydia, lyme as well as various metabolic disorders such as toxic "gut" and diabetes. OK that's a big category. One might say I am being simplistic. BUT MAYBE IT IS JUST THAT SIMPLE. Whatever stresses the body in those individuals with a compromised vascular system may trigger the blood reflux into the CNS. Illness in childhood may damage the vascular system, stress including toxic stress may trigger the reflux. Toxicity itself may damage the veins. All these factors may stress the vascular system leading to a venous blood reflux. Detoxification, intestinal cleansing, and appropriate nutrition will reduce pressure on the vascular system as well as nurture the brain and heal nerve damage.
CURE: Some MS patients recover through diet cleansing and nutritional therapy alone. Some may have a "temporary" stress reaction to a toxic substance such as aspartame (or mercury in dental almagam fillings.) The reaction is "temporary" in the sense that once the toxin is removed, the MS symptoms disappear. I have even heard that removing glutens from the diet is sufficient to heal.
CONTROL: Dr. Terry Wahls (see You Tube Minding Your Mitochondria) presents another excellent example. She began her treatment by de-toxifying from the MS drugs which were poisoning her and then optimized her nutrition. Her recovery implies that her veins were not actually blocked, but tensed up enough to cause a reflux. Also, she stimulated her blood circulation by electrical stimulation of the bands of muscles on her back, in other words, the bladder meridian. Optimal Diet/Supplements serve two purposes. 1) to prevent stress on the vascular system which might lead to blood reflux and 2) heal damaged tissue.
In addition to nutritional therapy, most MS patients probably will require treatment to enhance blood circulation to prevent blood refluxes – massage, ayervedic massage, acupuncture, self acupressure, osteopathy, chiropractic, swimming.
Again, to make a long story short, Dr. Zamboni has discovered the problem – venous blood reflux or CCSVI – but not the sole solution. Detoxification and nutritional therapy coupled with circulation therapies and/or skeletal adjustments may suffice without taking the risk of angioplasty.
MS Cure Enigmas.net
Post subject: Re: Five CCSVI MS Types
Re: DrSclafani answers some questions
Hi Dr S, good questions above ;)
Dr has the flow testing of the Total flow changes from CCSVI been compared with the early studies that showed that PwMS had something like 20-50% less blood flow through the brain.
It seems that the original figures had the impact required to make people consider that total flow was an issue, what I would like to hear is what impact CCSVI is having compared to the original data of 20-50% less and also if the symptoms regress what impact does that have on these figures, do the figures regress also?
It seems that this hasn't been done?
Is there any news on Paulo's collar as yet,
I would still Love to buy the system and travel the Country to show both Patients and Dr's/Specialists that these are issues to be addressed!
Regards,
Nigel
Dr has the flow testing of the Total flow changes from CCSVI been compared with the early studies that showed that PwMS had something like 20-50% less blood flow through the brain.
It seems that the original figures had the impact required to make people consider that total flow was an issue, what I would like to hear is what impact CCSVI is having compared to the original data of 20-50% less and also if the symptoms regress what impact does that have on these figures, do the figures regress also?
It seems that this hasn't been done?
Is there any news on Paulo's collar as yet,
I would still Love to buy the system and travel the Country to show both Patients and Dr's/Specialists that these are issues to be addressed!
Regards,
Nigel
-
drsclafani

- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
That is a great question. The answer would be very complex, and require quite a bit of thought. So a pat five line answer won"t do it. Let me sleep on this one for a while. please pose the question at the new year. I think that will be a fitting time to look back. Since i do not sleep very much, i will need that much time to formulate my reply.EJC wrote:Dr S.
I follow this thread, despite not understand a reasonably large amount if it, I do try.
The fact you're here and spend the time discussing this subject in such detail with your patients and anyone else wanting to ask questions is simply outstanding, like you haven't got enough on your plate already. What I'm trying to find though is an overview of your thoughts. Not particularly just medical detail, but how you feel about where you are with CCSVI and where CCSVI is with MS patients.
Do you feel you understand CCSVI more than ever or as you've delved deeper into the subject are you still raising more questions than answers?
When you see a new patient do you feel a CCSVI procedure stands a good chance of helping them?
My wife had CCSVI treatment in Scotland in Dec 2010 and had very promising results (particularly eyesight improvements) which gradually regressed over the next 9-12 months. In Dec 2011 she had jaw realignment work in London which I'm documenting on this forum, with fantastic results.
Each treatment/procedure had a direct effect on different symptoms.
CCSVI returned warmth to my wifes hands and feet, reduced cog fog and provided an instant and substantial improvement in eyesight. Much of this regressed.
Jaw realignment eradicated debilitating neuralgia in her left arm, hand leg and foot. It also has reduced substantially the amount of fatigue she suffered from a daily "battery" life of awake hours of 6-7 hours to a near normal 12-14 hours. Rather than any sign of these regressing they are continuing to improve as time passes, to a degree that phyio and physical rehabilitation has begun to get her back on her feet and more mobile (EDSS reached 6.5 but now starting to improve).
As a layman I look at these results and see two treatments offering relief of two clear sets of symptoms. These are the questions that run through my mind.
1. Was my wife under treated for CCSVI (quite rightly at the time) as we were in the early stages of the development of the treatment two years ago?
2. Have we actually found two things my wife needed treating for but gone about it in the wrong order?
3. Is there any connection at all between skeletal misalignment/TMJ disorders and CCSVI? Or have we simply discovered my wife has two separate ailments providing symptoms currently known to medicine as MS?
4. Once treatment for My wifes TMJ problem are complete would she benefit from a further CCSVI procedure based on the initial improvements of the first procedure?
I'm not actually sure I even expect an answer, I'm typing this more to share my thoughts rather than look for something definitive. But I would really like to know where you feel you are at the moment with CCSVI, globally. In laymans terms.
TIA.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re: DrSclafani answers some questions
I actually re read what I wrote after I'd posted it. It then dawned on me that what I'd asked probably required the equivalent of a 2 to 3 hour presentation with slides.drsclafani wrote: That is a great question. The answer would be very complex, and require quite a bit of thought. So a pat five line answer won"t do it. Let me sleep on this one for a while. please pose the question at the new year. I think that will be a fitting time to look back. Since i do not sleep very much, i will need that much time to formulate my reply.
I'll bump my post in January and see if you've got the first chapter put together.
Looking forward to it
EJC.
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
DarrenLuvsadonut wrote:EJC,
As Im unsure which treatment to go for first (had a positive CCSVI scan at Glasgow 2 years ago and an appointment with Dr Amir tomorrow) I follow your threads as much as possible, therefore even without an answer from Dr S, I appreciate your thoughts. That said I too would love to hear Dr Sclafanis thoughts on the connection/possibility of CCSVI/TMJ/MS.
Darren
I dont have an opinion about the sequence of treatments. I am not that familiar or expert in the cervical adjustment techniques, their validity or their outcomes. I can only speak about what I am expert in. My rendering an opinion about skeletal alignment is like a neurologist discussing the safety and technique of venoplasty and venography. Dont expect me to throw my weight on the subject without expertise.
All patients I see have a minimum of two venous outflow obstructions. Those obstructions alter venous flow throughout the cerebral and paravertebral venous pathways and have effects on cerebrospinal and arterial flow. Whether problems in one system supersede another is unclear to me. Having an opinion means little. the research data will answer the question.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
It is unclear whether one procedure supersedes the other. I fail to see how realignment does anything to manage a stenosis of a vein that results in venous obstruction of the inferior jugular bulb. Moreover, i fail to see how treating venous obstruction does anything for CSF obstructions at the skull base.EJC wrote:Hello Darren,
I was having a chat with another patient of Amir's last week whilst sat in the waiting room. She was going through the same thought process.
Actually she'd been to See Dr S earlier this year and is now seeing Amir, she felt with hindsight, like us that she'd probably do the two things the other way around. Get the skeleton sorted, then if you still have issues maybe go the CCSVI route.
I was lying on bed the other night and it was then that it struck me how the two different procedures were dealing with completely separate symptoms.
I know Amir reads this thread and absorbs the vast amount of information that Dr S writes to see if it can in some way help him with what he does. I figured I may as well ask Dr S for his thoughts too.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
Thinking about the first three years of CCSVI management, i have noted with alarming frequency some of the errors that were made commonly by proceduralists. Today a very disappointing story illustrated this and points to some explanations for many of the fleeting improvements that many patient experience after angioplasty
The patient was a middle aged Canadian woman with relapsing remitting MS that had progressed into the secondary stage. Her symptoms included chronic debilitating fatigue, temperature intolerance, imbalance, problems with memory and cognition, numbness and tingling and weakness in the extremities and bladder difficulties.
In 2010 she was treated in a European facility. The venogram was interpreted as showing valvular stenosis of the left internal jugular vein at the inferior jugular bulb, and incorrectly diagnosed a normal right internal jugular vein and normal azygous vein. The angiography was poor with very minimal contrast media. However to my eye, valvular stenoses of both the right IJV and the Azygous arch were clearly evident. Angioplasty of the left IJV was performed with a stent that was too small for that vein. Not surprisingly follow up venography was interpreted as showing inadequate angioplasty. Instead of increasing balloon size, stenting was performed. The patient was given a few days of anticoagulation and discharged. some of her symptoms improved, others did not and then some of the improvements regressed.
In 2011 she went to another facility in Europe and imaging was repeated. This second interventionalist detected the right IJV valvular stenosis and treated that successfully. Extensive intimal hyperplasia of the stented left IJV had developed and this has resulted in a narrowing of the lumen in the stent by about 70%. The Left IJV was treated by angioplasty of the stent without additional stenting. Azygous venography again was misinterpreted as normal and again left untreated. Surprisingly, left renal venography was also performed. I saw reflux into the left ovarian vein and was consistent with the renal vein compression syndrome. No intervention was performed.
most would consider this patient to have failed venoplasty. In reality this has just been unsatisfactory treatment. it has take three session to diagnose the critical pathology and some of the lesions still have not been treated. Moreover an unnecessary stent has been ultilized and this will likely lead to a chronic stenosis of the left IJV
hopefully i can address some of these problems tomorrow
The patient was a middle aged Canadian woman with relapsing remitting MS that had progressed into the secondary stage. Her symptoms included chronic debilitating fatigue, temperature intolerance, imbalance, problems with memory and cognition, numbness and tingling and weakness in the extremities and bladder difficulties.
In 2010 she was treated in a European facility. The venogram was interpreted as showing valvular stenosis of the left internal jugular vein at the inferior jugular bulb, and incorrectly diagnosed a normal right internal jugular vein and normal azygous vein. The angiography was poor with very minimal contrast media. However to my eye, valvular stenoses of both the right IJV and the Azygous arch were clearly evident. Angioplasty of the left IJV was performed with a stent that was too small for that vein. Not surprisingly follow up venography was interpreted as showing inadequate angioplasty. Instead of increasing balloon size, stenting was performed. The patient was given a few days of anticoagulation and discharged. some of her symptoms improved, others did not and then some of the improvements regressed.
In 2011 she went to another facility in Europe and imaging was repeated. This second interventionalist detected the right IJV valvular stenosis and treated that successfully. Extensive intimal hyperplasia of the stented left IJV had developed and this has resulted in a narrowing of the lumen in the stent by about 70%. The Left IJV was treated by angioplasty of the stent without additional stenting. Azygous venography again was misinterpreted as normal and again left untreated. Surprisingly, left renal venography was also performed. I saw reflux into the left ovarian vein and was consistent with the renal vein compression syndrome. No intervention was performed.
most would consider this patient to have failed venoplasty. In reality this has just been unsatisfactory treatment. it has take three session to diagnose the critical pathology and some of the lesions still have not been treated. Moreover an unnecessary stent has been ultilized and this will likely lead to a chronic stenosis of the left IJV
hopefully i can address some of these problems tomorrow
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re: DrSclafani answers some questions
Honesty,
I Love it, this is what creates Learning!!!!!!!!!!!
Thanks Sal
I Love it, this is what creates Learning!!!!!!!!!!!
Thanks Sal
Re: DrSclafani answers some questions
Some thoughts about how neck alignment could help in MS
The misalignment is due to muscle spasm and muscle "shortening" .The only reason is the vein congestion of the muscles
This muscle spasm, is temporarily reduced by neck alignment
I personally had it the other way around
I had neck pain and back pain for years (maybe it was my first MS symptom) and x-rays always showed a strange position of my neck vertebrae, i also had two mild hernias
I was relieved from this pain after my angioplasty on June 2011 (please Cece, would you bump up the pictures and discussion page 414?)
Performed a new MRI recently, the MS lesions were inactive, the hernias were milder (!) but also the profile x-ray of my neck revealed a normal posture of my vertebrae.
The whole posture of my body is normal now.
This excellent results of the angioplasty were followed by physical exercise. After all those years of muscle spasm, the muscles need exercise and physiotherapy to extent and work again normally.
It's the muscles that lead to misalignment.
The misalignment is due to muscle spasm and muscle "shortening" .The only reason is the vein congestion of the muscles
This muscle spasm, is temporarily reduced by neck alignment
I personally had it the other way around
I had neck pain and back pain for years (maybe it was my first MS symptom) and x-rays always showed a strange position of my neck vertebrae, i also had two mild hernias
I was relieved from this pain after my angioplasty on June 2011 (please Cece, would you bump up the pictures and discussion page 414?)
Performed a new MRI recently, the MS lesions were inactive, the hernias were milder (!) but also the profile x-ray of my neck revealed a normal posture of my vertebrae.
The whole posture of my body is normal now.
This excellent results of the angioplasty were followed by physical exercise. After all those years of muscle spasm, the muscles need exercise and physiotherapy to extent and work again normally.
It's the muscles that lead to misalignment.
getafix
Re: DrSclafani answers some questions
Yup, that's why we're all here throwing suggestions around, trying to understand how all these things interact, or even if they interact at all.drsclafani wrote: It is unclear whether one procedure supersedes the other. I fail to see how realignment does anything to manage a stenosis of a vein that results in venous obstruction of the inferior jugular bulb. Moreover, i fail to see how treating venous obstruction does anything for CSF obstructions at the skull base.
I have a feeling (and that's all it is as I have no medical training whatsoever) the Emma was under treated for CCSVI in Scotland, simply because more is now understood. The Canadian lady discussed above is an example of what I think occurred, fortunately we decided to have no stents in the original procedure.
However, as Emma is now undergoing skeletal and jaw misalignment treatments it would be logical to complete that before considering anything else. There's also the small matter of finding another $10,000 or so for another procedure.
Would we do it differently in hindsight? Probably, we'd do the skeletal stuff first. That may simply be due to hindsight, or the realisation that CCSVI is still (or was) in it's infancy in 2010 when Emma was treated.
Does one come before the other? I have no idea, if there's a correct order of treatment that assumes the two "conditions" actually interact, that's another big assumption.
Re: DrSclafani answers some questions
EJC,
I found your question #3 to be curious. Never having been diagnosed with TMJ,(I have seen a specialist) I seemed to have symptoms.
My jaw had been locked for approx. 4yrs. causing (right side) inner ear , jaw, and neck pain. I had embolization done and the following day, my jaw unclenched and there is no more pain. I did have CCSVI procedures, but they never improved my jaw. I don't know if it's a coincidence, but it is interesting.
I believe changes/improvements should be noted.
I found your question #3 to be curious. Never having been diagnosed with TMJ,(I have seen a specialist) I seemed to have symptoms.
My jaw had been locked for approx. 4yrs. causing (right side) inner ear , jaw, and neck pain. I had embolization done and the following day, my jaw unclenched and there is no more pain. I did have CCSVI procedures, but they never improved my jaw. I don't know if it's a coincidence, but it is interesting.
I believe changes/improvements should be noted.
Re: DrSclafani answers some questions
Wishing you dramatic success in this.drsclafani wrote:hopefully i can address some of these problems tomorrow
The azygous and renal vein stenoses have never been treated, the right jugular has successfully been treated, and the left jugular is compromised with the stent and no longer able to achieve the optimal treatment that was originally possible in the naive vein.
If the left jugular is compromised like this, then it would seem to be more important than in patients with healthy jugulars on both sides that the venous sinuses communicate freely. When you check the sinuses, are you able to identify this, or are you only seeing the entry to the sinus on each side? There was a research study in healthy controls that the venous sinuses did not communicate freely in about 50%; that has stuck with me as an issue needing eventual consideration especially given the one-sided occlusion of jugulars in some patients. I am not sure how "communicating freely" is precisely defined. I have seen images here where contrast is released in one jugular and travels through the sinuses and out the other jugular.
Re: DrSclafani answers some questions
this is what you're looking for, pelopidas?drsclafani wrote:glad you are a poster child for ccsvi. you are a lucky one. not everyone has such great responses. but it could not happen to a nicer woman.pelopidas wrote:I had a terrible chronic neck pain and occipital headache (in the back of my head) for the past 7-8 years.
MRI showed some mildly prolapsed cervical disk, so i thought i would live with it forever. I was having physiotherapy and i was taking pain killers almost every second day.
Then, 6 months ago (6/10/2011) i had my angioplasty procedure.
One month later i was talking to Dr Sclafani about the great improvements i already had. I mentioned that my neck pain was unexpectedly disappeared. He replied only "Ah, it was the spasm!"
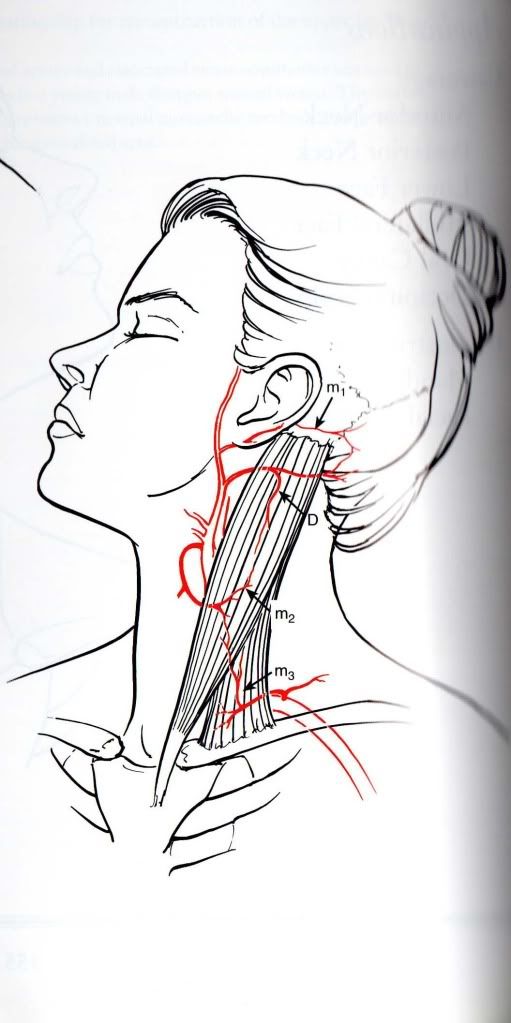
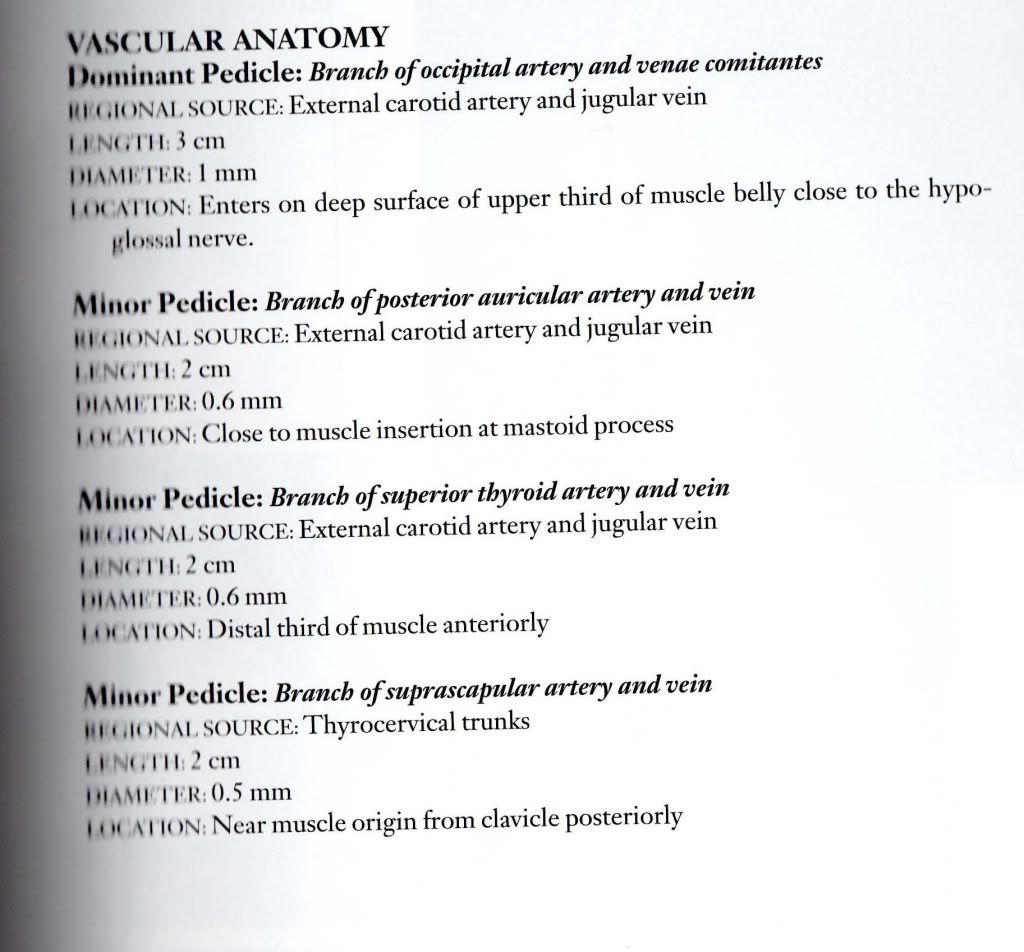
I found what he meant:
this is the anatomy and the vessels of the sternocleidomastoid muscle (only the arteries here, the veins were of no importance until recently)
almost 90% of this pair of muscles has venous outflow through the jugulars
Maybe the spasm was some symptom of venous congestion of the muscles.
I am relieved of the neck pain and i can turn and flex my head so easily now.
I hope that this will last forever and so will all my other improvements.
Maybe other people have experienced the same thing.
Muscles have veins, too!
Thank you again Dr Sclafani (and this one is a special 6 months post-op thank you)!
-and thank you Cece for the image uploading advice!
a hint on sharing images on TIMS: dont use URL, use. This command will push the image directly into your email. your audience will not have to press on the link. see your image by my technique. They show directly in the post.
very interesting hypothesis regarding reduction of neck pain.what about this consideration: patients with MS often havfe very large condylar emissary veins that connect to the veins in the posterior neck. Could relieving the resistance in the IJV, reduce flow through the emissary vein and thus reduce venous congestion in the neck muscles?
Sal
In infants, stenosis in the internal jugular vein can lead to congestion and clotting in the small veins of the neck muscles which leads to scar tissue in the neck muscle which leads to torticollis. So what Dr. Sclafani says about internal jugular stenosis potentially leading to congestion of the neck muscles is plausible and supported in torticollis research.
Re: DrSclafani answers some questions
Outstanding is a good word for it. Remarkable, surprising, appreciated? I would not have the knowledge I have if it weren't for what has been taught here.EJC wrote:I follow this thread, despite not understand a reasonably large amount if it, I do try.
The fact you're here and spend the time discussing this subject in such detail with your patients and anyone else wanting to ask questions is simply outstanding, like you haven't got enough on your plate already.
EJC, you and someone else made a comment recently about not understanding everything here. I couldn't find the other comment. I was wondering what parts aren't being understood?
-
- Similar Topics
- Replies
- Views
- Last post