
Dr S, I am glad all went well with your #1 fan, Cece
Cece's turn
I am in such sympathy with you over the three children. As you know, I also have three children to care for, and as a parent going solo I have always felt a huge responsibility with the MS -- both in being there for them and in choosing treatments. I feel so emotional for you going through this. You wrote that this should be available for everyone. That was also my conviction after experiencing my procedure. Aside from any measurable effect on EDSS, I felt so much more *alive* and life was so much more vivid. I felt a combination of grief for the years I had missed, personally and with my children, and joy for what could be possible, for me and for my family and for other people who could experience this procedure.
It was truly a life-changing experience. I am happy beyond words for anyone who can do this. And I am grateful beyond words to the doctors like Dr. Sclafani who dedicate themselves to us and to the advocates who work to make it possible. Don't think that something as simple as vivid vision or a "reduction in fatigue" can't change someone's life and mean just as much as a point on an EDSS scale!
And to anyone who thinks that needing to have this more than once means it's a failure -- on the contrary, it is a brilliant success that anything, anything can bring us back into the kodachrome world. Like when Dorothy steps out of the black and white wrecked house into multicolored OZ and realizes she's way, way over the rainbow. Now *that* is a fine place to be.
It was truly a life-changing experience. I am happy beyond words for anyone who can do this. And I am grateful beyond words to the doctors like Dr. Sclafani who dedicate themselves to us and to the advocates who work to make it possible. Don't think that something as simple as vivid vision or a "reduction in fatigue" can't change someone's life and mean just as much as a point on an EDSS scale!
And to anyone who thinks that needing to have this more than once means it's a failure -- on the contrary, it is a brilliant success that anything, anything can bring us back into the kodachrome world. Like when Dorothy steps out of the black and white wrecked house into multicolored OZ and realizes she's way, way over the rainbow. Now *that* is a fine place to be.
-
girlgeek33

- Family Elder
- Posts: 150
- Joined: Thu Nov 26, 2009 3:00 pm
- Location: NJ
- Contact:
CeCe! This is great news!!! I'm so happy you have joined the Liberati!!!
I have had this done 3 times. My last procedure last month with Dr. Sclafani & Smitty. First two with Dr. Bonn. After the first procedure, I went full steam ahead and enjoyed every bit of my new found health. In hind sight, not the best thing to do. This time, I followed every bit of medical advice and took it easy for 2 weeks following the procedure. And the suggestion to drink lots of plain water is another great one to follow.
I look forward to hear all about all of your improvements as you begin to notice them in the coming weeks! All my best to you!
Denise
I have had this done 3 times. My last procedure last month with Dr. Sclafani & Smitty. First two with Dr. Bonn. After the first procedure, I went full steam ahead and enjoyed every bit of my new found health. In hind sight, not the best thing to do. This time, I followed every bit of medical advice and took it easy for 2 weeks following the procedure. And the suggestion to drink lots of plain water is another great one to follow.
I look forward to hear all about all of your improvements as you begin to notice them in the coming weeks! All my best to you!
Denise
What does Dr. Sclafani think of this? I had one bad jug with pretty good collaterals, but my azygous was a mess. I had little to no cogfog or fatigue, but a nasty spinal cord lesion and associated disability.Cece wrote:It is interesting, isn't it. There is the question of why, with near complete blockage of one jugular and absolute complete blockage of the other, why did I not climb the EDSS chart like a mountaineer. I had bad jugular CCSVI but "mild" MS. Mild in quotes, because of the cogfog and severe fatigue and plenty of hindrances to full living. But nothing needed ballooning in the azygous, that is why I did not have spinal lesions and that sort of disability?
I am glad you've had such a great result. If you figure out how not to be paranoid about restenosis, let me know as this is a daily struggle for me. Don't tell Dr. Sclafani but this might be something for which faith is more useful than science.
Cece
Congratulations on finally getting the procedure! I wish you a successful and complete recovery. My prayer for you is that MS will become just a bad memory, and will no longer affect your life. It sounds like you're on the right track.
My appologies for coming to the party so late. I was just away from the forum for a few days and all this excitement happens!
Congratulations on finally getting the procedure! I wish you a successful and complete recovery. My prayer for you is that MS will become just a bad memory, and will no longer affect your life. It sounds like you're on the right track.
My appologies for coming to the party so late. I was just away from the forum for a few days and all this excitement happens!
-
CenterOfGravity
- Family Member
- Posts: 47
- Joined: Fri Oct 01, 2010 2:00 pm
Cece, It's so great to hear how you are doing! Follow that advice and rest up and drink water!! (I'm filing it all away in my brain for when I do it!).
Reading this made me sad to think of how much farther things would be if neurologists were actually helping instead of hindering the process of discovery and research when it comes to CCSVI. In making the connection, wouldn't it be great if the IRs and the neuros could genuinely work together to try to make correlations between types of CCSVI, and where lesions are and what type of disability? Asking the IRs to do that is as unreasonable as it is to ask a neuro to have a clinical trial or research study to diagnose CCSVI using any technique, as it isn't their specialty. I do feel confident that while it may take a few years, like the whole h.pylori story, things will move in the right direction, and we WILL see big changes. I know I feel such gratitude to the doctors and patients and advocates who are the pioneers in this!Jugular wrote:What does Dr. Sclafani think of this? I had one bad jug with pretty good collaterals, but my azygous was a mess. I had little to no cogfog or fatigue, but a nasty spinal cord lesion and associated disability.Cece wrote:It is interesting, isn't it. There is the question of why, with near complete blockage of one jugular and absolute complete blockage of the other, why did I not climb the EDSS chart like a mountaineer. I had bad jugular CCSVI but "mild" MS. Mild in quotes, because of the cogfog and severe fatigue and plenty of hindrances to full living. But nothing needed ballooning in the azygous, that is why I did not have spinal lesions and that sort of disability?
-
cheerleader

- Family Elder
- Posts: 5361
- Joined: Mon Sep 10, 2007 2:00 pm
- Location: southern California
Congrats, Cece. You've been working hard and have been a terrific advocate for others, as well as yourself.
You and Jeff presented almost identically---he had a 99% closure of the left IJV, and a 85% closure of the right, yet was mobile and walking with 20 brain lesions. Dr. Dake said the same thing....looking at his MRI and MRV, he was astounded that Jeff was not more disabled. He actually said, he wondered how he walked across the room. But Jeff's fatigue, cog fog, depression and heat intolerence were disabling him.
Cerebral disability does not always present in mobility issues. And I agree with COG..this is why we need neurologists and radiologists understanding how hypoperfusion can harm the brain. Jeff's fatigue wasn't "all in his head"...but it was all in his head. I know you understand now.
Continued hydration, rest, deep breathing and healthy eating. Enjoy the HDTV vision
hope and healing,
cheer
You and Jeff presented almost identically---he had a 99% closure of the left IJV, and a 85% closure of the right, yet was mobile and walking with 20 brain lesions. Dr. Dake said the same thing....looking at his MRI and MRV, he was astounded that Jeff was not more disabled. He actually said, he wondered how he walked across the room. But Jeff's fatigue, cog fog, depression and heat intolerence were disabling him.
Cerebral disability does not always present in mobility issues. And I agree with COG..this is why we need neurologists and radiologists understanding how hypoperfusion can harm the brain. Jeff's fatigue wasn't "all in his head"...but it was all in his head. I know you understand now.
Continued hydration, rest, deep breathing and healthy eating. Enjoy the HDTV vision
hope and healing,
cheer
Husband dx RRMS 3/07
dx dual jugular vein stenosis (CCSVI) 4/09
http://ccsviinms.blogspot.com
dx dual jugular vein stenosis (CCSVI) 4/09
http://ccsviinms.blogspot.com
-
CCSVIhusband
- Family Elder
- Posts: 475
- Joined: Sun Jun 27, 2010 2:00 pm
- Location: Pittsburgh, PA USA
- Contact:
Again, I'll echo everyone else, but say that you now know what I've been going on about with the "personal experience".
And now that you have that experience, I'm sure you'll be more convinced than ever the role CCSVI plays ... and be a stronger advocate for others.
You've done a lot of great work on TIMS ... and I look forward to that continuing as well as being able to relate it to your own personal stories now that you know what the rest of the CCSVIers know.
And now that you have that experience, I'm sure you'll be more convinced than ever the role CCSVI plays ... and be a stronger advocate for others.
You've done a lot of great work on TIMS ... and I look forward to that continuing as well as being able to relate it to your own personal stories now that you know what the rest of the CCSVIers know.
-
drsclafani

- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Yes CeceCece wrote: If Dr. Sclafani is so inclined, perhaps he will post the images from the procedure today, so that everyone can see the before-and-afters and admire his handiwork? It was exactly as it should be afterwards, free-flowing and wide open.
My azygous too is of interest, it was enormous. It would seem to have been recruited to help drain the brain as the blood was going down the verts then through the azygous instead of directly through the jugulars.
He was able to use fairly large balloons. I believe my right was 16 mm as measured by ivus, so he oversized by 2 mm with an 18 mm balloon, which showed two waists if I overheard correctly. On the left it was smaller, but not by much.
I am now tired, a little overwhelmed by the odd sights/sounds, and with a sore neck, but very pleased with how things went, and as always impressed with Dr. Sclafani's skills and kindness.
although you have a copy of the images, perhaps it would be good for you and your fans to review here as you suggest.
The sequence was as follows
1. prep and drape
2. time out
3. cath in left femoral under local anesthesia
4. advancement into right jugular, venogram, ivus, 18 mm angioplasty to thirteen atmospheres, repeat venogram
5. advancement into left jugular, venogram, ivus, angiopasty to 14 mm at ten Atm, repeat venogram
6. advancement into azygous vein, venogram of ascending azygous followed by zero, twenty, seventy and ninety degree views of the azygous arch
7. IVC venogram
8 ascending lumbar venogram
images as follows
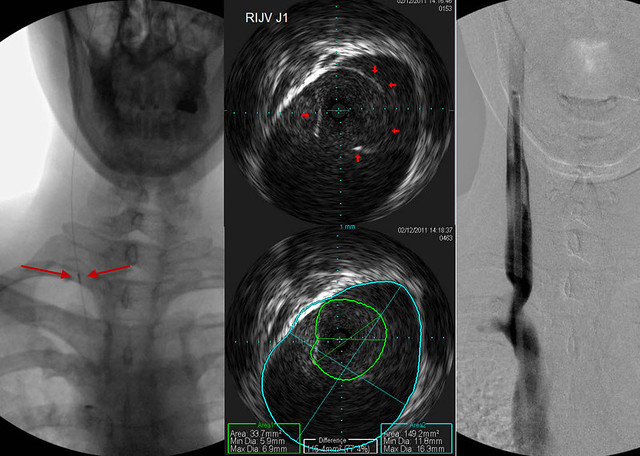
This sequence shows the ivus probe on the far left of the screen at the point where these images were taken. The venogram is on the right shows a bad stenosis.
My goal has become to stretch the narrowing as much as possible without stretching the area of normal vein above it. That is a great value of the IVUS.
The IVUS images are in the middle. they show that there is a fused or stuck valve at the area of narrowing (outlined in red arrows). The IVUS can show us the cross sectional area of the narrowed segment and compare it to the normal segment automatically. The IVUS measurements of the diameter are precise to a tenth of a millimeter and of the cross sectional area of a 100th of a square millimeter.

This set of images is from a bit higher in the vein where there is a transition in diameter of the vein (Left image red arrows). The two IVUS images in the center are at exactly the same location. One shows almost no lumen to the vessel, measurning less than 3 millimeters. When Cece breathed deeply out, it is clear that this is not a stenosis but a phasic narrowing, much like what happens when any healthy person is upright. It does not need to be dilated and dilation will likely have no effect. Unfortunately such narrowings sometimes end up being stented. The IVUS helps me differentiate a fixed stenosis from a physiological narrowing.
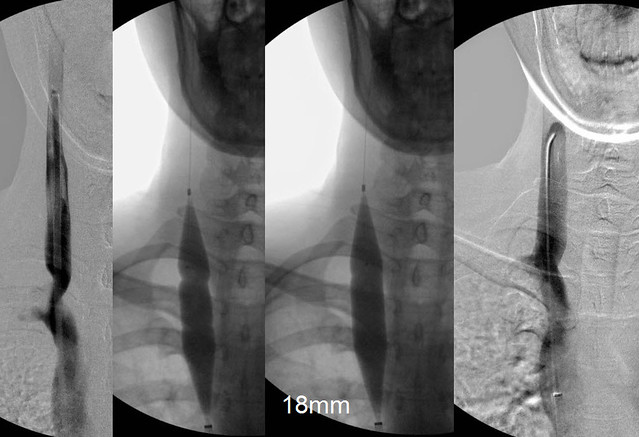
This third sequence shows the venoplasty images. There are two narrowings, the upper of the two was more obvious and probably represented one set of malformed valves. The lower one is less pronounced. This might have been a normal or nearly normal second set of valves. This can happen.
The final image on the right is post venoplasty. I like that the vein is wide open without any bulge of the normal vein above the stenosis. Hopefully it will reduce the risks of restenosis or thrombosis.

This image is a venogram of the left side. I didnt see any reason to show another IVUS but it was similar to that on the right side. These images show a very tight stenosis of almost 100%. There are vertebral collaterals seen. These vertebral collaterals can drain through the vertebral veins into the subclavian vein but because of chronic obstruction some of this drainage can travel through the vertebral plexuses that are continuous down the spine. So some of the drainage goes from the plexuses into the intercostal and lumbar veins and out into the azygous system.

This final sequence shows the very large and smooth azygous vein and its collaterals through the veno cava and the ascending lumbar vein.
Cece was a great patient. She held her breath in the proper position and phase of respiration to obtain maximum imaging.
She even laughed at my jokes
Last edited by drsclafani on Sun Feb 13, 2011 3:00 pm, edited 1 time in total.
-
Vivianne766

- Family Elder
- Posts: 190
- Joined: Sun Mar 07, 2010 3:00 pm
- Location: WNY
- Contact:
-
CCSVIhusband
- Family Elder
- Posts: 475
- Joined: Sun Jun 27, 2010 2:00 pm
- Location: Pittsburgh, PA USA
- Contact:
Are you saying such narrowings "should be" stented - if they don't hold up to angioplasty? And in this specific case, is it likely a stent MAY be needed in the future?drsclafani wrote:
This set of images is from a bit higher in the vein where there is a transition in diameter of the vein (Left image red arrows). The two IVUS images in the center are at exactly the same location. One shows almost no lumen to the vessel, measurning less than 3 millimeters. When Cece breathed deeply out, it is clear that this is not a stenosis but a phasic narrowing, much like what happens when any healthy person is upright. It does not need to be dilated and dilation will likely have no effect. Often such narrowings end up stented.
OR are you saying such narrowings are often stented by other doctors ... but shouldn't have been in the first place?
OR are you saying something I'm missing the point to?
Are you coming around on the use of stents (if there were better stents) in some cases?