
Sir Sclafani,
Just wonderful to read your messages, thank you! About IVUS; sounds like wonderful tool for CCSVI research.. so is there comig research publications where data is "collected" with IVUS? And how valuable tool it is for you with CCSVI? There are quite many doppler studies with mixed results.. hopefully other imaging techniques give more and clear data.
DrSclafani answers some questions
-
tiredloulou

- Family Member
- Posts: 26
- Joined: Wed Jul 14, 2010 2:00 pm
- Contact:
medication, after ccsvi, Dr. S. question?
my follow up was to take 1 aspirin daily...........
no mention or script of plavix or?
since the only follow up is my family dr.
should I be requesting to be placed on plavix?
due to stent
and procedure..
no mention or script of plavix or?
since the only follow up is my family dr.
should I be requesting to be placed on plavix?
due to stent
and procedure..
Makes good sense. We've had a patient report here at TIMS of accidental femoral artery puncture and a report of femoral vein thrombosis.drsclafani wrote:the reasons are several
1. injury to the femoral vein has greater consequences
2. repeated punctures might lead to stricture.
3. always do the most bengn and less risky procedure.
4. the femoral vein is closer to the femoral artery

(apologies for multiple posts in a row, I am working through Dr. Sclafani's big post...)
In your previous pre-CCSVI experience, did you go into the sinuses? Very rarely?
Is it safe?
Excellent images, as always.
Is it just the guidewire that you would send across this way?drsclafani wrote:Initially the guidewire was advanced through the left jugular bulb into the sigmoid sinus. Then it was advanced across the transverse sinus, into the right sigmoid sinus and finally past the right jugular bulb and into the the jugular vein.
In your previous pre-CCSVI experience, did you go into the sinuses? Very rarely?
Is it safe?
Excellent images, as always.
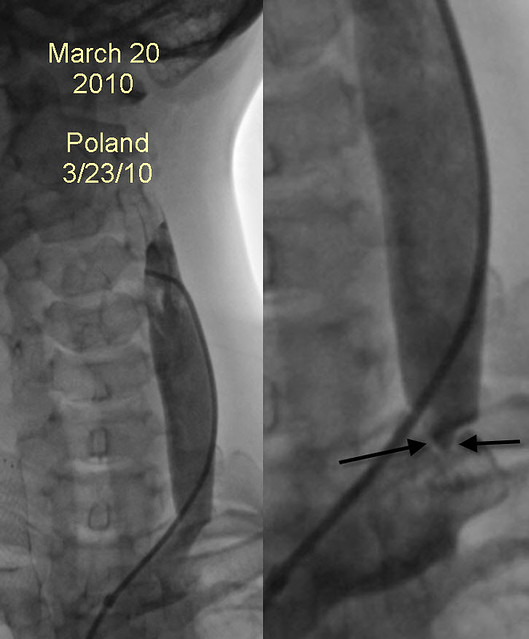
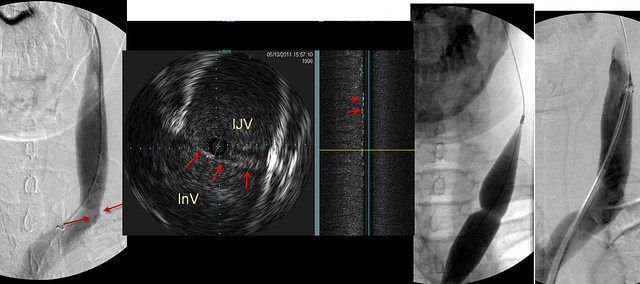
That seems very subtle on the IVUS image. Would it be easy to miss even on IVUS? Experience makes a difference?drsclafani wrote:before returning to the RIJV, left IJV venography was performed. It showed a subtle "jet" of contrast media (red arrows). Intravascular ultrasound showed a septum across the ostium of the left IJV at its entrance into the left subclavian vein. on the sagittal view, the septum was represented as scattered white lines (red arrow) on IVUS
Venoplasty clearly shows the "waist" on the balloon and after 14 atmosphered of pressure were applied, the "waist was no longer seen. I wonder whether this will also represent a challenge as Nunzio's left jugular was!
It looks good in the final image. Why do you think it might be a challenge? Was Nunzio's a septum too?
-
tiredloulou
- Family Member
- Posts: 26
- Joined: Wed Jul 14, 2010 2:00 pm
- Contact:
ccsvi- medication on follow up?
my ccsvi treatment was 6 months ago
1 stent
I just had ultra sound last follow up..........all appeared to be good( and it was the zamboni outline of ultra sound done in toronto
but, reading about the poor follow up's we do have, to none in canada
makes me wonder if I should request script from my fam. dr
the dr. who did ccsvi is in pacific interventionalist ......
and said, no need for anything.........except my aspirin
1 stent
I just had ultra sound last follow up..........all appeared to be good( and it was the zamboni outline of ultra sound done in toronto
but, reading about the poor follow up's we do have, to none in canada
makes me wonder if I should request script from my fam. dr
the dr. who did ccsvi is in pacific interventionalist ......
and said, no need for anything.........except my aspirin
UPPER MID: for all our talk of IVUS, it is always striking how tiny and cute it is.drsclafani wrote:The next image is a composite that summarizes the intervention done on the J3 segment of the RIJV
UPPER LEFT image shows contrast in the sigmoid sinus. However the upper jugular vein was not seen. Collaterals in the neck and spine were seen.
UPPER MID: A second wire was advanced as a safety wire and over it was placed an IVUS probe. (dark spot)
UPPER RIGHT: IVUS shows an occlusion of the upper jugular vein. Measurment of diameters of occlusions is not easy by venography, but IVUS is quite precise (YELLOW ARROWS).
LOWER LEFT & MIDDLE: 8mm by 6cm angioplasty performed. However there was no flow on angiography.
LOWER RIGHT: Therefore a stent was placed8mm by 4cm. Venography shows flow.
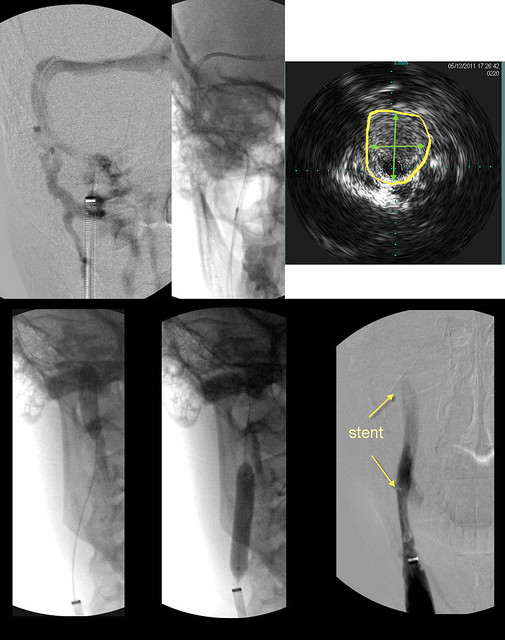
UPPER RIGHT: Dr. Cumming had a post the other day which really drove home the precision of IVUS, he posted an image where the vein looked narrowed on venogram and would've been treated by some doctors but on IVUS it was an oval-shaped vein with far greater area than it had appeared to have because it was seen in the venogram straight-on at the narrow end of the oval.
LOWER LEFT & MIDDLE: Why did the vein not respond to the angioplasty? Previously would you have chosen to go bigger and higher pressures on this stenosis?
LOWER RIGHT: It's the patient's third procedure; IVUS was used and it was a true occlusion not physiological; this occlusion was resistant to angioplasty; she'd tolerated the previous stent well albeit with mild intimal hyperplasia; as you said, there was no flow, it was entirely occluded. Still I think of patients who have ended up with occluded high-up stents. I would hate to be in the situation of having to decide this. You would make the same choice again, if a similiar situation presents itself?
Last edited by Cece on Tue May 17, 2011 6:38 pm, edited 1 time in total.
This is the web and not the persistent immobile valve?drsclafani wrote:Finally in the ascending azygous vein i noted some funky looking echoes. These likely represent webs.
I am used to ivus images of fixed valves, it is good to have a chance to see the septum earlier and this too.
I'm ready now for the Saturday storySo that the story of my patient and me on a late Friday night date.
Things i learned are that
1. prior treatments may not be durable
2. Early treatments overlook things
3. the entire jugular vein must be imaged
4. there is a role for stents
5. webs may be visible on IVUS
-
drsclafani

- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Cece, this was a special case trying to determine whether there was even a bony canal. the wire helped me see where the vein should be. It might also have been able to create a tract that allowed the right jugular catheter to be advanced.Cece wrote:(apologies for multiple posts in a row, I am working through Dr. Sclafani's big post...)
Is it just the guidewire that you would send across this way?drsclafani wrote:Initially the guidewire was advanced through the left jugular bulb into the sigmoid sinus. Then it was advanced across the transverse sinus, into the right sigmoid sinus and finally past the right jugular bulb and into the the jugular vein.
In your previous pre-CCSVI experience, did you go into the sinuses? Very rarely?
Is it safe?
Excellent images, as always.
in my pre ccsvi experience I NEVER went into the sinuses. There was no need. i have been giungerly tip toeing up there for about six months periodically. First i was sending the IVUS up there to explore, and then, after two stenoses of the dural sinuses were encountered, i have since been trying to place a catheter into the sigmoid sinus as the first part of the exam. The primary purpose has been to assure myself that the vein was intace, which it sometimes is NOT.
Today, i administered some fentanyl before doing it and preinstructed the patient about the weird sensation of bubbling water
I am not sure that the patient was entirely happy. I will find out more tomorrow
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
on the ivus there are all kinds of subtle echoes, the significance of each is still unclear to me. Initially i thought they were artefacts but as i see the sagittal IVUS i am becoming more convinced that these are real. What do do about them is not clear to me yet.Cece wrote:That seems very subtle on the IVUS image. Would it be easy to miss even on IVUS? Experience makes a difference?drsclafani wrote:before returning to the RIJV, left IJV venography was performed. It showed a subtle "jet" of contrast media (red arrows). Intravascular ultrasound showed a septum across the ostium of the left IJV at its entrance into the left subclavian vein. on the sagittal view, the septum was represented as scattered white lines (red arrow) on IVUS
Venoplasty clearly shows the "waist" on the balloon and after 14 atmosphered of pressure were applied, the "waist was no longer seen. I wonder whether this will also represent a challenge as Nunzio's left jugular was!
It looks good in the final image. Why do you think it might be a challenge? Was Nunzio's a septum too?
I wonder because this patient has now had two angioplasties. one balloons with buddy wires, the other at high pressure.
Each failure i have is always a source of angst for me
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: ccsvi- medication on follow up?
that is wonderful. six month followup is a very positive sign but remember that zamboni reported that the majority of restenosis occured from 8-14 months after treatment. Hopefulfly the PI patients will continue to show improved technical success with larger balloons.tiredloulou wrote:my ccsvi treatment was 6 months ago
1 stent
I just had ultra sound last follow up..........all appeared to be good( and it was the zamboni outline of ultra sound done in toronto
but, reading about the poor follow up's we do have, to none in canada
makes me wonder if I should request script from my fam. dr
the dr. who did ccsvi is in pacific interventionalist ......
and said, no need for anything.........except my aspirin
i think, that you should follow your doctors recommendations. If you have questions, you should ask them their philosophy practice and results.
i think asking a family doctor instead of your IR makes no sense. Why not have your family doctor do the procedure. f
I have found that it is more difficult but no impossible to stay in touch with my patients who come from many countries and states. Not all, mind you, both my problem and theirs, but as i develop an international practice, i am finding it not unreasonable to keep in touch as long as you can make connections with local doctors.
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Cece wrote:UPPER MID: for all our talk of IVUS, it is always striking how tiny and cute it is.drsclafani wrote:The next image is a composite that summarizes the intervention done on the J3 segment of the RIJV
UPPER LEFT image shows contrast in the sigmoid sinus. However the upper jugular vein was not seen. Collaterals in the neck and spine were seen.
UPPER MID: A second wire was advanced as a safety wire and over it was placed an IVUS probe. (dark spot)
UPPER RIGHT: IVUS shows an occlusion of the upper jugular vein. Measurment of diameters of occlusions is not easy by venography, but IVUS is quite precise (YELLOW ARROWS).
LOWER LEFT & MIDDLE: 8mm by 6cm angioplasty performed. However there was no flow on angiography.
LOWER RIGHT: Therefore a stent was placed8mm by 4cm. Venography shows flow.
UPPER RIGHT: Dr. Cumming had a post the other day which really drove home the precision of IVUS, he posted an image where the vein looked narrowed on venogram and would've been treated by some doctors but on IVUS it was an oval-shaped vein with far greater area than it had appeared to have because it was seen in the venogram straight-on at the narrow end of the oval.
LOWER LEFT & MIDDLE: Why did the vein not respond to the angioplasty? Previously would you have chosen to go bigger and higher pressures on this stenosis?
LOWER RIGHT: It's the patient's third procedure; IVUS was used and it was a true occlusion not physiological; this occlusion was resistant to angioplasty; she'd tolerated the previous stent well albeit with mild intimal hyperplasia; as you said, there was no flow, it was entirely occluded. Still I think of patients who have ended up with occluded high-up stents. I would hate to be in the situation of having to decide this. You would make the same choice again, if a similiar situation presents itself?
IVUS, CUTE?
YOUR FEMININE SIDE IS SHOWING
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
MY THOUGHT IS THAT THIS VEIN WAS DONE, FINITO, OF NO VALUE. IN LESS THAN ONE YEAR IT HAD BECOME TOTALLY BLOCKED. WHAT ALTERNATIVE IS THERE AT THIS POINT. aND IN A PATIENT WITH HORRIFYING SPASTICITY.Cece wrote:FROM THE IVUS, ONE CAN SEE THE CORRECT SIZE OF THE VEIN. DILATING MUCH ABOVE THE NORMAL VEIN SIZE WOULD SIMPLY RESULT IN RUPTURE AND ULTIMATE RETHROMBOSIS. THAT IS THE POWER OF IVUS. EVEN IN AN OCCLUSION, WHERE VENOGRAPHY DOES NOT SHOW THE LUMEN, WE CAN DECIPHER THE TRUE DIAMETER AND PROPERLY SIZE THE BALLOON.drsclafani wrote:The next image is a composite that summarizes the intervention done on the J3 segment of the RIJV
UPPER MID: for all our talk of IVUS, it is always striking how tiny and cute it is.
LOWER LEFT & MIDDLE: Why did the vein not respond to the angioplasty? Previously would you have chosen to go bigger and higher pressures on this stenosis?LOWER RIGHT: It's the patient's third procedure; IVUS was used and it was a true occlusion not physiological; this occlusion was resistant to angioplasty; she'd tolerated the previous stent well albeit with mild intimal hyperplasia; as you said, there was no flow, it was entirely occluded. Still I think of patients who have ended up with occluded high-up stents. I would hate to be in the situation of having to decide this. You would make the same choice again, if a similiar situation presents itself?
-
- Similar Topics
- Replies
- Views
- Last post