HappyPoet wrote:Hi Dr. Sclafani,
I'm puzzled by the reflux of contrast into the L-DS after venography of the R-TS. What path did the contrast take and what accounts for this reflux? Do you have video of this as it's happening that you can show (maybe youtube)?
Sorry, i dont have it. The dural sinuses for the most part are a continuous circuit of venous drainage that allows flow from one to the others. In this case the contrast flows from one transverse sinus to the other and then down into the left jugular vein Why would this happen? Because there is more resistance to flow on the same side as there is to the other side.
HappyPoet wrote:So, at this point in time, all appears well with the once-treated R-IJV. The once-treated L-IJV venous wall, though, appears intact, as if only temporarily stretched with too small a balloon--which accounts for both the temporary improvement in symptoms and no permanent injury to the vein wall above the stenosis. Could it be, though, that the vein wall, itself, was never dilated, that the balloon shoulder had been placed against just the valvular stenosis and not the vein wall at all, eccentrically ala Sclafani?
Yes that is possible. The problem is that the valvular stenosis was not effectively dilated to remain open for a long time. My point is twofold, choosing a balloon size that will adequately stretch the stenosis while minimizing the stretch of the normal vein.
HappyPoet wrote:How does the number of times the balloon is inflated and the length of time the balloon is inflated fit into the overall equation that also includes the atmospheres of pressure used/required and the size of balloon chosen, ala Sclafani IVUS Balloon-sizing Method discussed below?
frequency of inflation: each inflation imparts stress to the vein wall and the stenosis, sometimes several stretches allow gradual stress rather full stress during one inflation
duration of inflation
longer duration may allow prolonged stretch of the stenosis; however it increases the time that intimal gets no oxygen
amount of pressure applied
The more pressure the greater the forces applield to expand the tissue. Highly resistant tissues require higher pressure to stretch it
size of the balloon
balloon size determines how much stretch is applied. undersizing results in inadequate stretch, oversizing risks overwhelming the structure integrity of the structure
HappyPoet wrote:If a patient wanted a conservative procedure, is balloon sizing an area where a patient could ask for you to dilate only to a 50% increase in cross sectional area measurement as opposed to 80%?
I can only speak personally. I value my expertise and judgment. As such I am willing to hear patients' desires, but ultimately the physician should be responsible to meet the goal of the patient in a safe and responsible way. I would feel uncomfortable deferring years of training to the less educated directions of a patient. Actually there is the possibility of malpractice in certain situations.
Also it is my responsibility to educate my patients so that they understand what i am doing and why i am doing it
HappyPoet wrote:Where did you place the shoulder of the balloon? Was there a valve at the confluens? Was this decision difficult?
there are two shoulders upper and lower. I use both shoulders depending upon the anatomy. I try to place the majority of the balloon in the area that is largest so that there is less stretch on the balloon. For the most part the vein above the stenosis is usually smaller than below the stenosis. That means that I would place the upper shoulder at the stenosis and the rest of the balloon would trail into the larger more central vein. In those circumstances were the vein above was more dilated, i would use the lower shoulder at the stenosis and let the remainder of the balloon flop into the upper dilated segment.
HappyPoet wrote:Again, I'm puzzled. Will this angioplasty stop blood from flowing/refluxing down the L-DS and L-IJV?
If the obstructions at the valve are overcome and the resistance is reduced by enlargement of the stenosis sufficiently, then flow should go to the path of least resistance down the jugular.
This is the primary purpose of the angioplasties
HappyPoet wrote:By "annular narrowings," do you mean the two areas seen had an actual annulus with no valve flaps? Was there a "pop" heard when the annular narrowings went away?
annular stenosis is a bad term, sorry. Zamboni used it to describe a short focal circumferential stenosis. Ironic, then, that the majority of the stenoses occur at the annulus, which is the scaffold of hard collagen tissue that provides support for the attached valves
i no longer like to hear the pop...i try slower and repeated dilatations to stretch rather than fast. I have learned from my mistakes.

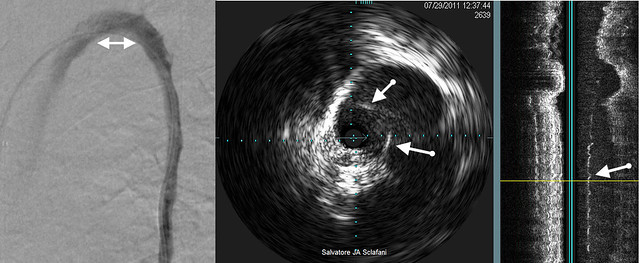
HappyPoet wrote:This shows the value of IVUS.
I honestly don't see anything on the sagital reconstruction where the arrow is pointing near the thin, green horizontal line. What does the large shift in signal represent far above the arrow?
the large shift represents movement of the tissue during normal breathing,and pulsations.
i would consider the green line to be vertical. It represents the plane of the ivus device. to the right of the green lines one sees some white longitudinal speckles. There represent sound reflections off the narrowed valvular area.
HappyPoet wrote:This makes sense; how does an IR tell the difference between thrombosis, and/or intimal hyperplasia, and/or valvular or intraluminal tissue that is either not staying pressed into the vein wall or is a defect?
All of this is VERY interesting. 
ultrasound can usually tell the difference. The hemodynamics might be misleading but the anatomical visualization is pretty good and one should be able to differentiate these problems for the most part.
HappyPoet wrote:Please forgive my cogfog, but I don't get this--what about restenosis?
in this case, i believe that this patient was undertreated rather than restenosed. I am just making the point that all instances where patient loses improvements are not the result of restenosis. Thus repeating procedures in this circumstance is essential and not an overzealous repeated angioplasty.
HappyPoet wrote:Thank you, DrS!
thank you. Your questions were very good. I am impressed.
i thank you because your questions and those of others have helped guide my thinking and formulate my answers to patients.