B+ to FHappyPoet wrote:Thank you, Cece.
Okay, I'll stick with my original answer (second-guessing myself is second-nature to me).
DrSclafani answers some questions
-
drsclafani

- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
F to B+HappyPoet wrote:The more I think about this case and look at this image, the more questions I have about my original answer...
My original answer doesn't explain why an IR would use a machine with that exact 'dark vertical line' problem being right where the R-IJV would be? I don't think an IR would use such a defective machine for the purpose of investigating the R-IJV. So this would mean that Pam's and Cece's original answers are correct, that the catheter traversed the sinuses which would mean that the wire did go through the heart and SVC which must be lower than this image shows? So if the 'dark vertical line" really is a catheter, I'm surprised at how stiff and straight it appears in this image... "peculiar" is the right word, Cece.
My original answer also doesn't explain the absence of the guidewire below the uninflated balloon in the L-IJV which means the balloon had to have been threaded down from the sinuses, correct? Where else could the wire and balloon have come from? Unless the wire broke at the bottom of the balloon after it had been threaded up high in the L-IJV or even into the dural sinuses?
Cece, what say you?
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
Yespelopidas wrote:..is it inside the patient' s body?
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
It would be great to get the IVUS probe to do that but it often is not possible to get the probe to go up one jugular canal and down the other side.CD wrote:I think the L IJV had a lower blockage, perhaps at the junction, so this was the only way to enter the L IJV was by going up the R IJV then across and down to the L IJV to clear a blockage that way. JMO
The dye was not released, so maybe IVUS was looking around the L IJV first.
What say you teacher?
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com

Re: DrSclafani answers some questions
Perhaps due to a completely blocked and impenetrable LIJV that was inaccessible from the proximal side (taking proximal to mean from the heart side)?drsclafani wrote:Correct. Why would i do that?pklittle wrote:The catheter advanced through the sheath, up the right jugular, across the transverse sinus, and down the left jugular?
NHE
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: Dural sinus are safe with DrS
Lest the CCSVI world now spread a story that DrSclafani uses the Liberation Procedure as a recreational tool, let me end the rumor that the procedure room in Brooklyn, New York is my personal Disneyworld. I love m y work, but it ain't a game.MarkW wrote:HappyPoet wrote: I am not comfortable with the idea of having anything in my dural sinuses if my dural sinuses cannot be visualized the entire time. Period.
DrS accessed my dural sinuses in June 2011. A little painful at the time but no after affects. Depends if you want a full diagnosis or not and approach to risk, personal choice.
To answer DrS's 'why would I do that ?' Do you suspect a web and this is to help diagnosis ?
Of course it could be to develop your skills/because you can/because its fun.............
MarkW
I would never do this for fun. I recall the first time the wire accidentally went into the dural sinuses during a procedure. Depends would have come in handily at that moment. I was quite cautious and tried to avoid entering catheter or guidewire into the dural sinuses for my first 100 patients. I didn't have this excellent wire at the time. the larger stiffer wire was not suitable. And I was just damn cautious.
But there are very real reasons to place the guidewire into the dural sinus
1. to assure that your catheter is in the internal jugular vein. The catheter can enter branches of the jugular vein and mimic hypoplasia. I think that the only way to assure that you have seen the entire jugular vein is to opacify the veins from the dural sinus into the jugular vein. I have seen many cases sent by patients in which only the lower half or 2/3 of the IJV was opacified. My early procedures were very much like that too.
2. to assure that there is no stenosis of the dural sinuses. I cannot fully assess venous outflow obstructions without seeing the main intracranial vein draining the brain. Remember that the dural sinus and the IJV are one continuous circuit. The skull grows around these veins. If there is a hypoplasia of the vein entering the bony canal, it cannot be enlarged.
3. to perform IVUS in the dural sinus . This is useful in detecting stenosis of the dural sinus
4. to get a wire into the jugular vein (helping to identify the origin of the IJV on the opposite side). Helpful in occlusions, helpful in difficult catheterizations
5. in evaluating the condylar emissary vein and understanding the collateral drainage into the upper spine. (ok, this is conjecture but a worthy one.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
correctomundo!NHE wrote:Perhaps due to a completely blocked and impenetrable LIJV that was inaccessible from the proximal side (taking proximal to mean from the heart side)?drsclafani wrote:Correct. Why would i do that?pklittle wrote:The catheter advanced through the sheath, up the right jugular, across the transverse sinus, and down the left jugular?
NHE
The goal of this case is to really show a tale of two occlusions. I will continue but this train of discussion was going nicely today. Amazing how a single image that is at variance from the expected, can generate such discussion and touch on some very good points.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
MarkW

- Family Elder
- Posts: 1167
- Joined: Thu Oct 19, 2006 2:00 pm
- Location: Oxfordshire, England
- Contact:
Apology to DrSclafani
DrS,
I am sorry about my post:
"Of course it could be to develop your skills/because you can/because its fun............"
I travelled from Oxford, England to Brooklyn, New York because you are cautious in your diagnostic and treatment methods for CCSVI syndrome. I trust the patient mentioned is happy that you detected two occlusions, which most IRs would have missed.
MarkW
I am sorry about my post:
"Of course it could be to develop your skills/because you can/because its fun............"
I travelled from Oxford, England to Brooklyn, New York because you are cautious in your diagnostic and treatment methods for CCSVI syndrome. I trust the patient mentioned is happy that you detected two occlusions, which most IRs would have missed.
MarkW
Mark Walker - Oxfordshire, England. Retired Industrial Pharmacist. 24 years of study about MS.
CCSVI Comments:
http://www.telegraph.co.uk/news/health/8359854/MS-experts-in-Britain-have-to-open-their-minds.html
CCSVI Comments:
http://www.telegraph.co.uk/news/health/8359854/MS-experts-in-Britain-have-to-open-their-minds.html
-
MarkW
- Family Elder
- Posts: 1167
- Joined: Thu Oct 19, 2006 2:00 pm
- Location: Oxfordshire, England
- Contact:
Re: DrSclafani answers some questions
DrS wrote the info below. The simple message is that "unless your dural sinuses have been checked, stenoses could have been missed in the IJVs."
MarkW
DrS wrote : ...there are very real reasons to place the guidewire into the dural sinus
1. to assure that your catheter is in the internal jugular vein. The catheter can enter branches of the jugular vein and mimic hypoplasia. I think that the only way to assure that you have seen the entire jugular vein is to opacify the veins from the dural sinus into the jugular vein. I have seen many cases sent by patients in which only the lower half or 2/3 of the IJV was opacified. My early procedures were very much like that too.
2. to assure that there is no stenosis of the dural sinuses. I cannot fully assess venous outflow obstructions without seeing the main intracranial vein draining the brain. Remember that the dural sinus and the IJV are one continuous circuit. The skull grows around these veins. If there is a hypoplasia of the vein entering the bony canal, it cannot be enlarged.
3. to perform IVUS in the dural sinus . This is useful in detecting stenosis of the dural sinus
4. to get a wire into the jugular vein (helping to identify the origin of the IJV on the opposite side). Helpful in occlusions, helpful in difficult catheterizations
5. in evaluating the condylar emissary vein and understanding the collateral drainage into the upper spine. (ok, this is conjecture but a worthy one.
MarkW
DrS wrote : ...there are very real reasons to place the guidewire into the dural sinus
1. to assure that your catheter is in the internal jugular vein. The catheter can enter branches of the jugular vein and mimic hypoplasia. I think that the only way to assure that you have seen the entire jugular vein is to opacify the veins from the dural sinus into the jugular vein. I have seen many cases sent by patients in which only the lower half or 2/3 of the IJV was opacified. My early procedures were very much like that too.
2. to assure that there is no stenosis of the dural sinuses. I cannot fully assess venous outflow obstructions without seeing the main intracranial vein draining the brain. Remember that the dural sinus and the IJV are one continuous circuit. The skull grows around these veins. If there is a hypoplasia of the vein entering the bony canal, it cannot be enlarged.
3. to perform IVUS in the dural sinus . This is useful in detecting stenosis of the dural sinus
4. to get a wire into the jugular vein (helping to identify the origin of the IJV on the opposite side). Helpful in occlusions, helpful in difficult catheterizations
5. in evaluating the condylar emissary vein and understanding the collateral drainage into the upper spine. (ok, this is conjecture but a worthy one.
Mark Walker - Oxfordshire, England. Retired Industrial Pharmacist. 24 years of study about MS.
CCSVI Comments:
http://www.telegraph.co.uk/news/health/8359854/MS-experts-in-Britain-have-to-open-their-minds.html
CCSVI Comments:
http://www.telegraph.co.uk/news/health/8359854/MS-experts-in-Britain-have-to-open-their-minds.html
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
I treated my first referral from Dr. Franz Schelling. I am very honored.
Patient initially underwent venography at another facility which patient said was interpreted as normal. I found bilateral valvular stenosis 88% on right and 80% on left.
Patient initially underwent venography at another facility which patient said was interpreted as normal. I found bilateral valvular stenosis 88% on right and 80% on left.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: Apology to DrSclafani
MarkMarkW wrote:DrS,
I am sorry about my post:
"Of course it could be to develop your skills/because you can/because its fun............"
I travelled from Oxford, England to Brooklyn, New York because you are cautious in your diagnostic and treatment methods for CCSVI syndrome. I trust the patient mentioned is happy that you detected two occlusions, which most IRs would have missed.
MarkW
i fully know that you did not mean to convey the thought that i am frivolous. You and I have great respect for each other
my comment was more to make commentary about rumors on the internet
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
correctomundo!NHE wrote:Perhaps due to a completely blocked and impenetrable LIJV that was inaccessible from the proximal side (taking proximal to mean from the heart side)?drsclafani wrote:Correct. Why would i do that?pklittle wrote:The catheter advanced through the sheath, up the right jugular, across the transverse sinus, and down the left jugular?
NHE
The goal of this case is to really show a tale of two occlusions. I will continue but this train of discussion was going nicely today. Amazing how a single image that is at variance from the expected, can generate such discussion and touch on some very good points.[/quote]
The first patient is a 54 year old caucasian american male currently SPMS initially diagnosed in 1979.
He underwent treatment in January 2011.

these are images of the two venograms performed in January. The initial study is on the left three panels and shows an angioplasty of a lesion that is not well seen. A week later there is extensive thrombus in the LIJV.
In the patient's own words:
" My previous two procedures were done ....in early January. ... During the second procedure it was found that my LIJ had clotted (no stent). I was put on Lonenox, but had a bad reaction to it (wasn’t able to stay on it), was put on warifin immediately for 3 months. I finished up the warifin on April 12th, on that day I had an US and it showed I had flow in my jugulars, but they couldn’t tell me how much flow. They sent me home....
I ended up having a flare up of my MS during the 1st week of May, weaker legs and fatigue. I was put on 3 days of solumedrol with a 12 day pill taper. I was just starting to feel very good at the end of May when I ended up having another major flare, leg weakness, chest pressure, shortness of breath, heat in back and lack of bladder control (just felt like crap). I ended up in the ER twice. They ruled out everything ….must be the MS. My neurologist sent me for a spine MRI (looked clean, no active lesions). He put me on another 3 days of solumedrol on May 27th with another 12 day taper. I’m just starting to feel better the last couple of days, just getting back to work today. I’ve never had to do back to back steroid treatments. Well needless to say this has been one of the worse years of my life so far."
When he consulted me, i learned of the thrombosis so I was preparing to address this issue. A surface ultrasound confirmed the thrombosis. I began a complete diagnostic venogram but very quickly abandoned attempts to catheterize this vein from the femoral side of the catheterizationand went on to direct puncture of the high portion of the IJV via ultrasound guidance.
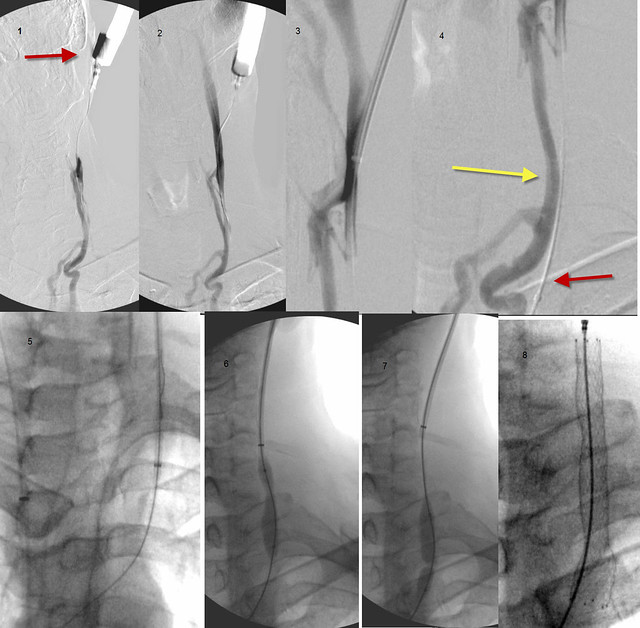
in window 1 you can see the red arrow pointing to the neck catheterization.
in window 4 most of the contrast material is opacifying the anterior jugular vein (yellow arrow) . You can see how it parallels the IJV (red arrow)
Bridging the thrombosis with a guidewire is the most important and often the most difficult component of this procedure. I used a guidewire first but it just kept getting hung up on this organized thrombus. Next i used a stiffer wire with a J on the tip to atraumatically push the wire through the clot. In this case this technique worked.
If it didnt work, then I would use the stiffer back end of a wire to push through the clot. If that failed, i would use a cutting needle IF i could assure myself that I was properly lining up the vein on both sides. This is often very challenging because there are adjacent structures such as lung, arteries, sometimes bowels (not in this situation) and other structures that might be injured if the alignment of the needle and the target was not perfect.
Another newer technique is radiofrequency delivery of heat energy to burn through the organized clot. However risks of perforation occur with this technique as well.
Thankfully, i was able to get the wire into the more central vein. and then i predilated the wire track. Next I used a snare to grab a wire from the femoral side and pull it through the thrombosis. Now with the wire across the thrombus, i was able to deploy some stents, and then balloon them (not shown) against the vein wall to get a good seal.

These images show an IVUS (center) to assure myself of a good apposition between stent and vein wall and nice IVUS (right) and venographic (left) images showing restoration of flow and diameter.
Lets discuss this and I will show the other case later.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re: DrSclafani answers some questions
If the thrombus was just one week old and it was caught, what options were there at that time?drsclafani wrote:
these are images of the two venograms performed in January. The initial study is on the left three panels and shows an angioplasty of a lesion that is not well seen. A week later there is extensive thrombus in the LIJV.
These are very interesting images. There is a visible collateral in the fourth panel. It definitely looks like the blood flow had worsened from the patient's initial baseline. The thrombus itself always looks like a thumbprint smudge.
The lesion is not well seen in the first panel, but there is definite waisting in the second panel. It is also in the usual area of the valves. The balloon may be large for the size of the vein, I can't really tell. It looks as if there was a good improvement in flow in the third panel. The images are very dark in places, I think more contrast dye was used than I am used to seeing.
Re: DrSclafani answers some questions
"In this case, it was possible to advance the wire from one transverse sinus to the other. You are correct. There was an occlusion of the right left jugular vein that occured from a prior procedure by another physician. By using the wire, i was trying to create a landmark that was definitely in the internal jugular vein. If I were lucky, i might be able to advance the wire down into the left innominate vein. "
So you have just invented the "retrograde ccsvi venogram"?
We all hope that you will publish soon all these , you promised that!
So you have just invented the "retrograde ccsvi venogram"?
We all hope that you will publish soon all these , you promised that!
getafix
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
1. anticoagulationCece wrote:If the thrombus was just one week old and it was caught, what options were there at that time?drsclafani wrote:
these are images of the two venograms performed in January. The initial study is on the left three panels and shows an angioplasty of a lesion that is not well seen. A week later there is extensive thrombus in the LIJV.
2. thrombolysis
3. thrombectomy
4. Stenting
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
- Similar Topics
- Replies
- Views
- Last post