That is easier said than done. Many patients have already had an abdominal ct scan and the renal vein compression is usually quite visible in retrospectCece wrote:Were you ever checked for Nutcracker, HP? It can be diagnosed with noninvasive doppler ultrasound ( http://www.ajronline.org/content/172/1/39.abstract )HappyPoet wrote:Very interesting. Could a lesion at a certain level, therefore, be an indication of possible Nutcracker syndrome and at what level would that be? Do you think IJV blockages alone could force reflux to travel below that level? At what levels are her spinal lesions?
Also, a related personal question: I have new T5/T6 lesions, yet my IJVs (PTA one year ago) and Azygos are fine; going by Dr. Schelling's theory, any ideas where refluxed blood to those cord levels might be coming from?
Very sorry to hear about the new lesions.
DrSclafani answers some questions
-
drsclafani

- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
It is my opinion that symptoms like fatigue, imbalance, weakness should be considered signs of Nutcracker, possibly even renal vein obstruction in a patient with MS should be considered nutcracker SYNDROME rather than the fairly ubiqitous nutcracker PHENOMENONHappyPoet wrote:Cece, thanks, I didn't know DUS can diagnose NS. Originally, I had been thinking along the lines of webs or septums being inside the hemiazygos as a possibility for the new lesions. Although I don't seem to have any symptoms of NS, for peace of mind, I'll ask to be checked for it at my next follow-up DUS.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re: DrSclafani answers some questions
An image is worth a thousand words...I would trade these twenty words for an image, if one or more were forthcoming?drsclafani wrote:I might add that IVUS of the vertebral vein was exciting. It showed anatomy wonderfully and did confirm suspected abnormalities
More please.drsclafani, to pelopidas wrote:you are correct. the vertebral is the one on the right. Why a catheter in it....in good time
HappyPoet, if you are seeing the talented Dr. Siskin for follow-ups, I don't expect you'll get anywhere asking about the renal vein. He has said he is waiting for the investigators who are looking at the renal vein to provide evidence.

Re: DrSclafani answers some questions
Cece, I forgot to mention that my next follow-up DUS will be with DrS (I saw Dr. Siskin for a follow-up DUS when I couldn't travel to NYC at the time).
DrS, I've had debilitating fatigue for over ten years, and left leg weakness (back of entire thigh) arrived with my current exacerbation. Are these enough signs of possible NS for you to order imaging of my left renal vein during my follow-up DUS? My symptom improvements (one year post-PTA) are still holding strong.
DrS, I've had debilitating fatigue for over ten years, and left leg weakness (back of entire thigh) arrived with my current exacerbation. Are these enough signs of possible NS for you to order imaging of my left renal vein during my follow-up DUS? My symptom improvements (one year post-PTA) are still holding strong.
Re: DrSclafani answers some questions
Ok, so my left jugular ended up being #1, and was better served by being treated twice than risking injury to the vein by going too far in a single procedure.drsclafani wrote:I also look forward to this opportunity. i can think of a few possible planned second procedures:
1. a highly resistant stenosis requiring very high pressures might be better suited to a planned second procedure rather than going overboard.
2. a questionable dissection, leading to an early ultrasound and second procedure
3. detection of an initially unrecognized lesion that is seen in retrospect after patient leaves the proceduree
4. an overly long procedure might be suspended with anticipated return.
I have to be judicious with this because the company still needs to at least make some profit to justify continuing the program. It is a for profit company.
We also will have a half priced policy for subsequent procedures. I will try to work out a technique that uses the data from the initial IVUS so that we can avoid the cost of the IVUS.
Yes, this really excites me. Compassionate care is important to me. Having patients worry about whether they can afford repeat procedures which many will need, is heartbreaking.
#2, in the event of a questionable dissection, would being able to do a second procedure mean that you are less likely to place a stent in such a dissection? Dissections are rare, aren't they?
Has #3 happened to you?
And I know #4 has happened! We have heard of the five hour procedures.
Re: DrSclafani answers some questions
DrS,
Best wishes at the SIR conference this weekend!

Best wishes at the SIR conference this weekend!
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
here you go, cece.Cece wrote:An image is worth a thousand words...I would trade these twenty words for an image, if one or more were forthcoming?drsclafani wrote:I might add that IVUS of the vertebral vein was exciting. It showed anatomy wonderfully and did confirm suspected abnormalitiesMore please.drsclafani, to pelopidas wrote:you are correct. the vertebral is the one on the right. Why a catheter in it....in good time
This is my first IVUS of a vertebral vein. The medical necessity for this IVUS was the fact that the internal jugular vein in J3 had long standing occlusion secondary to an overly aggressive angioplasty of a phasic compression of the IJV as it crosses the second vertebra. I saw some abnormality on the prior venogram and wanted to confirm my impression from the venogram that the vertebral had a valve and that it was thickened. I have read that the vertebral vein is valveless, but i think that is incorrect urban legend.
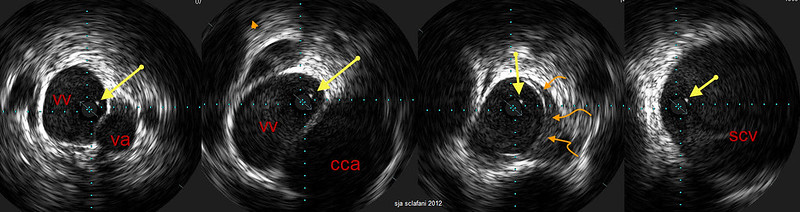
Four images
left: highest level before it turns into a vertebral plexus, which accounts for the tangles at the top of the venogram. this is in the bony canal with vertebral artery and vein nicely visible. on all four images one sees this echogenic dot (yellow arrows). I am thinking this is a web.
left middle: The vertebral artery is no longer seen. The larger common carotid artery is adjacent to this
right middle. Closer to the chest one sees the thickened valve that is immobile (curved orange arrows)
Right The vein is now entering the subclavian vein.
I performed a delicate vertebral vein angioplasty because the left IJV was occluded and not functioning.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
HappyPoet wrote:Cece, I forgot to mention that my next follow-up DUS will be with DrS (I saw Dr. Siskin for a follow-up DUS when I couldn't travel to NYC at the time).
DrS, I've had debilitating fatigue for over ten years, and left leg weakness (back of entire thigh) arrived with my current exacerbation. Are these enough signs of possible NS for you to order imaging of my left renal vein during my follow-up DUS? My symptom improvements (one year post-PTA) are still holding strong.
yes, i think so... but check to see if you have a body ct scan in the past. it would be a better anatomical study.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
Thanks. seven talks! i have never been so busy at a meetingHappyPoet wrote:DrS,
Best wishes at the SIR conference this weekend!
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re: DrSclafani answers some questions
http://www.ajnr.org/content/23/8/1418.short
Some support for the existence of vertebral venous valves!Ultrasonographic Evaluation of Vertebral Venous Valves
Chi-Hsiang Choua,
A-Ching Chaoa and
Han-Hwa Hua
From the Neurovascular Section, Neurologic Institute, Veterans General Hospital-Taipei, National Yang-Ming University, Taipei, Taiwan
Address correspondence to Professor Han-Hwa Hu, Neurologic Institute, Veterans General Hospital-Taipei, Taipei 11217, Taiwan
Abstract
Summary: To date, vertebral venous valves have not been studied clinically or by sonography. This report reveals that these valves could be studied noninvasively by using sonographic techniques. Real-time sonography clearly showed the opening and closing of the two cusps of vertebral venous valves at the junction of the vertebral vein and the brachiocephalic vein, which move synchronously with the internal jugular venous valves. This is the first time the vertebral venous valves have been studied by using clinical sonography. This might provide a new point of view for evaluating the clinical significance of vertebral venous valves.
Copyright © American Society of Neuroradiology
Re: DrSclafani answers some questions
Thanks. The images are even more interesting that I was expecting.drsclafani wrote:here you go, cece.
This is my first IVUS of a vertebral vein. The medical necessity for this IVUS was the fact that the internal jugular vein in J3 had long standing occlusion secondary to an overly aggressive angioplasty of a phasic compression of the IJV as it crosses the second vertebra.
It is painful to hear about an occlusion of an IJV due to an unnecessary treatment. (Assuming that phasic compressions are not treatable by angioplasty. And that ballooning the vein against a bone is asking for trouble.)
You've talked about the dots that may be webs, but never shown us such an example of one that can be seen throughout the vein, including images taken high in the neck and low in the neck. Really interesting and odd to see. I wonder if the other doctors who use IVUS regularly are also seeing dots.I saw some abnormality on the prior venogram and wanted to confirm my impression from the venogram that the vertebral had a valve and that it was thickened. I have read that the vertebral vein is valveless, but i think that is incorrect urban legend.
Four images
left: highest level before it turns into a vertebral plexus, which accounts for the tangles at the top of the venogram. this is in the bony canal with vertebral artery and vein nicely visible. on all four images one sees this echogenic dot (yellow arrows). I am thinking this is a web.
left middle: The vertebral artery is no longer seen. The larger common carotid artery is adjacent to this
right middle. Closer to the chest one sees the thickened valve that is immobile (curved orange arrows)
Right The vein is now entering the subclavian vein.
I performed a delicate vertebral vein angioplasty because the left IJV was occluded and not functioning.
Was the dot gone after the vein was ballooned?
That does look like a thickened valve. I think. But not a terribly big one? What percentage was the blockage? And, if you have time to answer, what did the vein measure for CSA at the area where it was ballooned? I am curious how it compares to the ballooning of a small IJV. I have a copy of a handy chart for looking up what balloon should be used, if CSA is known.
So the vertebral vein does enter the subclavian! I have been confused about the route.
-
elliberato

- Family Member
- Posts: 82
- Joined: Wed Aug 04, 2010 2:00 pm
- Contact:
Re: DrSclafani answers some questions
dr s,
I think youre amazing...im not blowing smoke up your behind. you talk about amazing discovery and technique, but with all due respect, and i mean due, i dont read much or can i find much about the improvements, which im sure are vast, in your patients? can you please share? thank you with all the respect in the world.
I think youre amazing...im not blowing smoke up your behind. you talk about amazing discovery and technique, but with all due respect, and i mean due, i dont read much or can i find much about the improvements, which im sure are vast, in your patients? can you please share? thank you with all the respect in the world.
Re:
*bumped for elliberato*drsclafani wrote:These are perhaps my ten most memorable reports from patients. they are not typical, for most patients have slight changes, that are sometimes pregressive improvements over time, others may not even be real. Other patients have never given me a followup
I ask all my patients now to send me a monthly email on their 'Liberation Day". hopefully many will do it so i can put what i do in perspective.
of course, i have said many times, my goal is to prolong time to disability. Everything else is a joyful surprise or a frustrating disappointment.
So here is the cases i will share with you
1. i its like all of a sudden someone took off my glasses and washed all the smudges off. But i wasnt wearing glasses.
2. i was so tired that i have never stood by the family bonfire as long as my kids can remember. Now i do. A few months later i am cross country skiing with my wife in the evenings.
3. I had a patient who was a wall walker, day after the procedure he came back and stood on one leg for what seems like a long time, and then rode a bicycle two weeks later.
4. i see in technicolor
5. I am less tired
6. I can harvest the winter wheat driving the combine and walk on the uneven terrain of the mud without falliing
7. nothing has changed
8 i feel worse, my balance is not as good
9.My feet are warm now
10. everything looks sharper and clearer
Re: DrSclafani answers some questions
WOW, In awe as always.
This is again big news that IVUS has found, with 'THE MAN' hanging on to it and reading the screen another reason for IVUS to be used, for eyes to be open and brain to not assume.
THANK YOU, Dr S
Bet your smiling as well and what a great way to change your career and make such a monumental difference in the world!
Thanks Dr,
Nigel
This is again big news that IVUS has found, with 'THE MAN' hanging on to it and reading the screen another reason for IVUS to be used, for eyes to be open and brain to not assume.
THANK YOU, Dr S
Bet your smiling as well and what a great way to change your career and make such a monumental difference in the world!
Thanks Dr,
Nigel
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
elliberato,elliberato wrote:dr s,
I think youre amazing...im not blowing smoke up your behind. you talk about amazing discovery and technique, but with all due respect, and i mean due, i dont read much or can i find much about the improvements, which im sure are vast, in your patients? can you please share? thank you with all the respect in the world.
I have always stated that I am not going to do a trial until I feel comfortable with my techniques, so i have focused on finding things that can cause problems, figuring out how to treat them effectively and safely, how to avoid major and minor problems, how to bale out of trouble, how to determine what can and cannot be done, what tests to do, etc.
Along the way I have done some good,seen some really amazing responses to treatment and had my share of disasters, and disappointments. I have helped many who were manhandled or misdiagnosed not because their doctors werent caring, but because patients seem to come to me when they are a bit desperate or things have gone badly during earlier treatments.
I find that more than 50% of my patients are progressive, a bit more advanced than Zamboni described in his papers. What are my results data. I honestly havent tried to do that yet. I have had to learn which tests to perform, how to perform then and how to interpret the results. While others seem to have people grading their MSIS, and MSQOL and Functional composites, i am going to have to do it myself. And i am gearing up to do that.
on the whole, i am feeling pretty good about what i am doing. Now, if only I could learn how to engage an academic neurologist who would partner with me treating patients
DrS
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
- Similar Topics
- Replies
- Views
- Last post