Dear Doctor,
if i'm not mistaken the LIJV had two stents in a row and the compression was just above the lower one. Do you know why the first IR chose to use two stents? Do you think that the compression could be avoided if the stents overlapped at the crucial point?
By ballooning inside a compressed stent, is there any damage done to the endothelial tissue surrounding the stent due to re-stretching of the metal mesh?
Regarding septa, are they routinely found in other parts of the body too? How/why do they form?
Regarding the ascending lumbar vein, you said it was very narrow. Could this be the result of inflammation due to the excessive retrograde flow from the left kidney?
What kind of stents do you use to treat the renal vein and how do you size their diameter and length?
DrSclafani answers some questions
-
drsclafani

- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
cece, actually, i do not think treatment is easy. While it is true that stenting has high long term patency in the renal vein, no doubt because of the torrential constant blood flow. However migration is always a risk. I have developed techniques that reduce this risk, but migration is always a risk in venous stenting because of the wide variation is vein size. No, I would not say that stenting the renal vein is a walk in the park!Cece wrote:An inflow vein of the cerebrospinal venous bed, when the cerebrospinal venous bed has enough flow and outflow obstructions of its own.
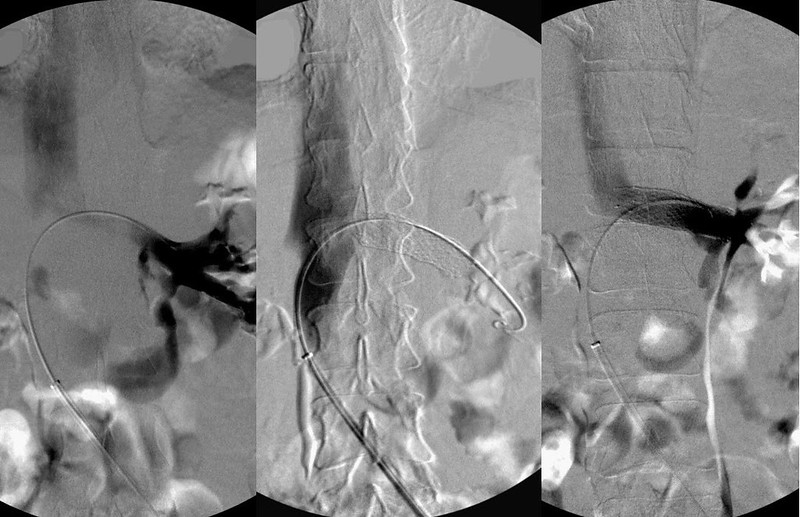
Nutcracker phenomenon results from compression of the left renal vein between the abdominal aorta and the superior mesenteric artery. The Left renal vein flows at about 550 ml/minute, which is 2-3 times the flow of both azygous and ascending lumbar veins combined. With outflow obstructions of the azygous and the ascending lumbar vein outflow, one can readily recognize the consequences of the renal vein obstruction as it converts the renal vein into an inflow vein of the cerebrospinal venous bed.
Treatment of this compressive obstruction is stenting. (image 3). Angioplasty alone is ineffective in reversing the renal vein compression.
It's so easily treated, too.
Last edited by drsclafani on Sat Jul 28, 2012 4:25 am, edited 1 time in total.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
I use self expanding nitinol stents.mo_en wrote:Dear Doctor,
What kind of stents do you use to treat the renal vein and how do you size their diameter and length?
I use ivus to calculate the cross sectional area of the renal vein from the kidney hilum to the inferior vena cava and measure the length of the vein from the renal hilum to the IVC. I want the stent to peek into the IVC and I want the other end of the stent to land just beyond the junction of the branch veins. I pick a stent that has about 20-25% larger in cross sectional area than the cross sectional area of the vein itself so that it is snuggly pressed against the vein wall. I want to use as long a stent as I can. This increases the amount of friction between the vein wall and the stent to resist migration. I deploy two stents because this will increase the hoop strength of the stent pushing against the nutcracker and make it stiffer to reduce bending .
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
I have not seen the images of the first angioplasty and do not know the indication for the stents. I suspect that compression of the vein by a cervical vertebral transverse process is the culprit. It is possible that overlapping the stents at that crucial spot may have increased the stiffness of that stent.mo_en wrote:Dear Doctor,
if i'm not mistaken the LIJV had two stents in a row and the compression was just above the lower one. Do you know why the first IR chose to use two stents? Do you think that the compression could be avoided if the stents overlapped at the crucial point?
I would think that would be the case. The endothelium is a layer of intimal cells with some fibrous tissue. Balloon dilation could scrape some off. That is one of the reason that anticoagulation and antiplatelet therapy are administered after angioplasty.By ballooning inside a compressed stent, is there any damage done to the endothelial tissue surrounding the stent due to re-stretching of the metal mesh?
Septums are walls dividing chambers or hollow structures.Regarding septa, are they routinely found in other parts of the body too? How/why do they form?
There are septums that separate the chambers of the heart. I have found several veins with septums, including the femoral veins, the iliac veins, the azygous vein, the internal jugular vein and the external jugular vein. I imagine they can occur in most veins. The are congenital variations [/quote]
Regarding the ascending lumbar vein, you said it was very narrow. Could this be the result of inflammation due to the excessive retrograde flow from the left kidney? [/quote]
That is a hypothesis of Dr T Scholbach
Med Hypotheses. 2007;68(6):1318-27. Epub 2006 Dec 11.
From the nutcracker-phenomenon of the left renal vein to the midline congestion syndrome as a cause of migraine, headache, back and abdominal pain and functional disorders of pelvic organs.
In it is reports that nutcracker has been associated with "neuropathies"
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re: DrSclafani answers some questions
Not wanting to distract the conversation.
Has anyone looked through this article by Dr Paul Thibault?
http://www.cosmeticcentre.com.au/client ... 043331.pdf
I posted this some back because I tested positive for CPn with the self test and a few days ago my Neuro has said she is not sure about my PPMS dx. I have had a few gallons of blood taken and have to go back for more to search for Lyme as well as a more reliable CPn test. I am waiting on her letter so I can critique her skills ;)
Keep smilin'
Nigel
Has anyone looked through this article by Dr Paul Thibault?
http://www.cosmeticcentre.com.au/client ... 043331.pdf
I posted this some back because I tested positive for CPn with the self test and a few days ago my Neuro has said she is not sure about my PPMS dx. I have had a few gallons of blood taken and have to go back for more to search for Lyme as well as a more reliable CPn test. I am waiting on her letter so I can critique her skills ;)
Keep smilin'
Nigel
-
newlywed4ever
- Family Elder
- Posts: 255
- Joined: Thu Apr 17, 2008 2:00 pm
- Location: Michigan
- Contact:
Re: DrSclafani answers some questions
Thanks for reposting the link, NZer - I missed it the first time around and now look forward to discussion.
-
blossom

- Family Elder
- Posts: 1394
- Joined: Thu Dec 03, 2009 3:00 pm
- Location: south western pa.
- Contact:
Re: DrSclafani answers some questions
nzer1--very very interesting. thanks for posting it. alas, the plot is thickening. looking forward to dr. sclafani's input.

Re: DrSclafani answers some questions
Does pregnancy possibly contribute to nutcracker syndrome of the renal vein? If so, one would expect a much greater occurrence of nutcracker in women. Is there any correlation supporting this hypothesis?drsclafani wrote:3. i am not aware of such a deleterious effect. I am also not sure that she restenosed. Possible explanation may have something to do with greater blood flow during pregnancy. perhaps it did something. otherwise, i have to wonder whether it was a red herring.Cece wrote:3. Is pregnancy known to contribute to restenosis in any other venous diseases?
NHE
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
cece, actually, i do not think treatment is easy. While it is true that stenting has high long term patency in the renal vein, no doubt because of the torrential constant blood flow. However migration is always a risk. I have developed techniques that reduce this risk, but migration is always a risk in venous stenting because of the wide variation is vein size. No, I would not say that stenting the renal vein is a walk in the park!drsclafani wrote:Cece wrote:An inflow vein of the cerebrospinal venous bed, when the cerebrospinal venous bed has enough flow and outflow obstructions of its own.
Nutcracker phenomenon results from compression of the left renal vein between the abdominal aorta and the superior mesenteric artery. The Left renal vein flows at about 550 ml/minute, which is 2-3 times the flow of both azygous and ascending lumbar veins combined. With outflow obstructions of the azygous and the ascending lumbar vein outflow, one can readily recognize the consequences of the renal vein obstruction as it converts the renal vein into an inflow vein of the cerebrospinal venous bed.
Treatment of this compressive obstruction is stenting. (image 3). Angioplasty alone is ineffective in reversing the renal vein compression.
It's so easily treated, too.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re: DrSclafani answers some questions
It is a bit much for me to sit at home with no IR training (other than what we're receiving here) and say that renal stenting is easy!
I would qualify however that at least in my mind, having been convinced that nutcracker when present is a contributor to CCSVI, the decision to get it treated and the decision of how it should be treated is straightforward.
That two doctors did not look for nutcracker in this patient is unfortunate and suggests that CCSVI patients would benefit from more awareness among the doctors of the relevance of nutcracker in CCSVI. And more publications and evidence in favor of treating nutcracker as well.
NHE, yes, nutcracker is more common in women in their third or fourth decade. http://www.phlebolymphology.org/2009/07 ... -syndrome/ I have been curious about the effect of the growing uterus on the compression of veins in the midsection. If my 9 lb babies compressed my bladder and my lungs, could they have compressed my azygous or renal vein too? But that would be for the duration of the pregnancy, not afterwards. Any abdominal weight gain due to the pregnancy could potentially worsen the compression of the renal vein. According to research posted during a previous discussion of nutcracker, nutcracker phenomenon was more likely to remain nutcracker phenomenon and not be nutcracker syndrome in patients who were young and skinny.
I would qualify however that at least in my mind, having been convinced that nutcracker when present is a contributor to CCSVI, the decision to get it treated and the decision of how it should be treated is straightforward.
That two doctors did not look for nutcracker in this patient is unfortunate and suggests that CCSVI patients would benefit from more awareness among the doctors of the relevance of nutcracker in CCSVI. And more publications and evidence in favor of treating nutcracker as well.
NHE, yes, nutcracker is more common in women in their third or fourth decade. http://www.phlebolymphology.org/2009/07 ... -syndrome/ I have been curious about the effect of the growing uterus on the compression of veins in the midsection. If my 9 lb babies compressed my bladder and my lungs, could they have compressed my azygous or renal vein too? But that would be for the duration of the pregnancy, not afterwards. Any abdominal weight gain due to the pregnancy could potentially worsen the compression of the renal vein. According to research posted during a previous discussion of nutcracker, nutcracker phenomenon was more likely to remain nutcracker phenomenon and not be nutcracker syndrome in patients who were young and skinny.
Re: DrSclafani answers some questions
Are renal vein valves a possible new direction of CCSVI research?
Renal Vein Valves: Incidence and Significance
Did you ever encounter a valve in the renal veins?
Renal Vein Valves: Incidence and Significance
Did you ever encounter a valve in the renal veins?
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
I have never encountered, or at least knew than i had encountered a valve in the renal vein. Until recently, I have only performed IVUS on patients whose renal venogram was suspicious for nutcracker phenomenon or syndrome. Recently I have been performing IVUS on all patients with CCSVI. I haven't seen a valve in the renal vein. But I think that i only see valves that are thickened, not normal valves. I will look more diligently for renal vein valves in the future.mo_en wrote:Are renal vein valves a possible new direction of CCSVI research?
Renal Vein Valves: Incidence and Significance
Did you ever encounter a valve in the renal veins?
DrS
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re: DrSclafani answers some questions
Hi,
Dr S I have been posting on all sorts of sites to get people talking and asking questions.
I have talked with Dr Paul Thibault in Sydney Australia over time about the viral and bacterial understandings he has about MS.
I have linked his comment about the Clinic he works for. They quote that they do CCSVI testing with doppler.
When asked;
" Hi Paul,
do you guys do Zamboni protocol Doppler assessments with a person trained by Zamboni?
* All the research is saying that there needs to be training from Zamboni? Is this your experience?"
the response was;
"Regarding the correctness of Zamboni's protocol, what research are you referring to Nigel? Also I don't see a link beteween cervical spine trauma and MS."
The other thing about people advertising and speaking on CCSVI treatments from Australia that I am astounded by is their refusal to acknowledge the benefit of IVUS.
How can this be educated, is it a case of Ego over Intelligence?
Regards,
Nigel
Dr S I have been posting on all sorts of sites to get people talking and asking questions.
I have talked with Dr Paul Thibault in Sydney Australia over time about the viral and bacterial understandings he has about MS.
I have linked his comment about the Clinic he works for. They quote that they do CCSVI testing with doppler.
When asked;
" Hi Paul,
do you guys do Zamboni protocol Doppler assessments with a person trained by Zamboni?
* All the research is saying that there needs to be training from Zamboni? Is this your experience?"
the response was;
"Regarding the correctness of Zamboni's protocol, what research are you referring to Nigel? Also I don't see a link beteween cervical spine trauma and MS."
The other thing about people advertising and speaking on CCSVI treatments from Australia that I am astounded by is their refusal to acknowledge the benefit of IVUS.
How can this be educated, is it a case of Ego over Intelligence?
Regards,
Nigel
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
nigel, i am not going to answer this question because it would serve no good purpose. . Not everyone is going to see things they way you do. Skepticism and doubt serve their purposeNZer1 wrote:Hi,
Dr S I have been posting on all sorts of sites to get people talking and asking questions.
I have talked with Dr Paul Thibault in Sydney Australia over time about the viral and bacterial understandings he has about MS.
I have linked his comment about the Clinic he works for. They quote that they do CCSVI testing with doppler.
When asked;
" Hi Paul,
do you guys do Zamboni protocol Doppler assessments with a person trained by Zamboni?
* All the research is saying that there needs to be training from Zamboni? Is this your experience?"
the response was;
"Regarding the correctness of Zamboni's protocol, what research are you referring to Nigel? Also I don't see a link beteween cervical spine trauma and MS."
The other thing about people advertising and speaking on CCSVI treatments from Australia that I am astounded by is their refusal to acknowledge the benefit of IVUS.
How can this be educated, is it a case of Ego over Intelligence?
Regards,
Nigel
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re: DrSclafani answers some questions
Thanks Dr S,
reminds me of watching teenagers looking in the fridge when their hungry, fridge is often full, they don't see food though?
Regards
Nigel
reminds me of watching teenagers looking in the fridge when their hungry, fridge is often full, they don't see food though?
Regards
Nigel
-
- Similar Topics
- Replies
- Views
- Last post