Will you be vanishing on an August trip anytime soon? I am not sure about this habit of taking vacations, wouldn't you rather be doing CCSVI?
DrSclafani answers some questions
Re: DrSclafani answers some questions
Any interesting cases lately, and any time to share them with us?
Will you be vanishing on an August trip anytime soon? I am not sure about this habit of taking vacations, wouldn't you rather be doing CCSVI?
Will you be vanishing on an August trip anytime soon? I am not sure about this habit of taking vacations, wouldn't you rather be doing CCSVI?
-
drsclafani

- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
i am working on a very interesting vignette right now. I hope to have it finished some time this weekCece wrote:Any interesting cases lately, and any time to share them with us?
Will you be vanishing on an August trip anytime soon? I am not sure about this habit of taking vacations, wouldn't you rather be doing CCSVI?
i am calllng it "Paradise lost, paradise regained". It will begin a discussion of early regression of clinical gains after ccsvi treatment
I will be going to the wilderness of northern new york state for a week soon. Given the number of questions, i dont think i will be missed too much.
actually i would prefer to do ccsvi but patients seem to like vacations too
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re: DrSclafani answers some questions
Dr. Sclafani,
You will be missed! But everybody needs a vacation.
In the case of CCSVI, if blood is taking longer to get to the heart, can this affect the heart rythm (Is it blood pressure)?
Sometimes my heart feels like it skips a beat or flutters fast. I notice this more when I restenose.
Also I was diagnosed 30 yrs. ago with mitral valve prolapse (no meds).
Thank you
You will be missed! But everybody needs a vacation.
In the case of CCSVI, if blood is taking longer to get to the heart, can this affect the heart rythm (Is it blood pressure)?
Sometimes my heart feels like it skips a beat or flutters fast. I notice this more when I restenose.
Also I was diagnosed 30 yrs. ago with mitral valve prolapse (no meds).
Thank you
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
mitral valve prolapse and MS: please read about ehlers danlos syndrome and see if it resonates with you.dlynn wrote:Dr. Sclafani,
You will be missed! But everybody needs a vacation.
In the case of CCSVI, if blood is taking longer to get to the heart, can this affect the heart rythm (Is it blood pressure)?
Sometimes my heart feels like it skips a beat or flutters fast. I notice this more when I restenose.
Also I was diagnosed 30 yrs. ago with mitral valve prolapse (no meds).
Thank you
MS can affect the heart rate and rhythm. This is more likely to be the cause than CCSVI itself.
DrSclafani
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com

Re: DrSclafani answers some questions
What about blood pressure? Mine seems to go up considerably during the night.drsclafani wrote:MS can affect the heart rate and rhythm. This is more likely to be the cause than CCSVI itself.
NHE
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
Since the brain stem has important regulatory function in maintaining blood pressure, MS can also result in high blood pressure although most patients seem to have lowish blood pressure.NHE wrote:What about blood pressure? Mine seems to go up considerably during the night.drsclafani wrote:MS can affect the heart rate and rhythm. This is more likely to be the cause than CCSVI itself.
NHE
S
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re: DrSclafani answers some questions
Might it be, that the brain is turning down blood pressure too protect it selfdrsclafani wrote:Since the brain stem has important regulatory function in maintaining blood pressure, MS can also result in high blood pressure although most patients seem to have lowish blood pressure.NHE wrote:What about blood pressure? Mine seems to go up considerably during the night.drsclafani wrote:MS can affect the heart rate and rhythm. This is more likely to be the cause than CCSVI itself.
NHE
S
Since the brain controlles the blood pressure it seems like a good way too minimize the damage????
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
This is an interesting proposal. In what way would lowering blood pressure minimize the damage. Can you imagine a way that lowering the blood pressure might be harmful.Ellegaard wrote:Might it be, that the brain is turning down blood pressure too protect it selfdrsclafani wrote:Since the brain stem has important regulatory function in maintaining blood pressure, MS can also result in high blood pressure although most patients seem to have lowish blood pressure.NHE wrote:
What about blood pressure? Mine seems to go up considerably during the night.
NHE
S
Since the brain controlles the blood pressure it seems like a good way too minimize the damage????
I appreciate your idea and would like to explore it further. thanks for participating
DrS
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re: DrSclafani answers some questions
S[/quote]
Since the brain stem has important regulatory function in maintaining blood pressure, MS can also result in high blood pressure although most patients seem to have lowish blood pressure.
S[/quote]
Might it be, that the brain is turning down blood pressure too protect it self
Since the brain controlles the blood pressure it seems like a good way too minimize the damage????[/quote]
This is an interesting proposal. In what way would lowering blood pressure minimize the damage. Can you imagine a way that lowering the blood pressure might be harmful.
I appreciate your idea and would like to explore it further. thanks for participating
DrS[/quote]
I guess that lowering the blood pressure, might be good for the brain, as the blocked veins is causing high blood pressure in the brain. But as for the rest of the human body constant low blood pressure is a bad situation, I geuss…
I btw have very low blood pressure myself, in spite of poor physical shape!
Sorry something went wrong with the quotes.
Greetings from Denmark
Mr. Ellegaard
Since the brain stem has important regulatory function in maintaining blood pressure, MS can also result in high blood pressure although most patients seem to have lowish blood pressure.
S[/quote]
Might it be, that the brain is turning down blood pressure too protect it self
Since the brain controlles the blood pressure it seems like a good way too minimize the damage????[/quote]
This is an interesting proposal. In what way would lowering blood pressure minimize the damage. Can you imagine a way that lowering the blood pressure might be harmful.
I appreciate your idea and would like to explore it further. thanks for participating
DrS[/quote]
I guess that lowering the blood pressure, might be good for the brain, as the blocked veins is causing high blood pressure in the brain. But as for the rest of the human body constant low blood pressure is a bad situation, I geuss…
I btw have very low blood pressure myself, in spite of poor physical shape!
Sorry something went wrong with the quotes.
Greetings from Denmark
Mr. Ellegaard
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
Ellegaard wrote:Might it be, that the brain is turning down blood pressure too protect it selfSince the brain stem has important regulatory function in maintaining blood pressure, MS can also result in high blood pressure although most patients seem to have lowish blood pressure. S
Since the brain controlles the blood pressure it seems like a good way too minimize the damage????
This is an interesting proposal. In what way would lowering blood pressure minimize the damage. Can you imagine a way that lowering the blood pressure might be harmful.
I appreciate your idea and would like to explore it further. thanks for participating
DrS
Greetings to you Mr. EllegaardI guess that lowering the blood pressure, might be good for the brain, as the blocked veins is causing high blood pressure in the brain. But as for the rest of the human body constant low blood pressure is a bad situation, I geuss…
I btw have very low blood pressure myself, in spite of poor physical shape!
Sorry something went wrong with the quotes.
Greetings from Denmark
Mr. Ellegaard
Actually, brain blood flow is often decreased in patients with MS, quite possibly due to decreased venous outflow. That being said, one would think that increasing pressure might allow more blood flow into the brain. However, increasing pressure also has some potentially negative consequences. Because cerebrospinal fluid (CSF) drainage is reduced, possibly as a consequence of decreased venous outflow, the pulsatility of arterial blood in-flow is not dampened and this may increase shear forces in the brain, which may injure the brain.
So it seems to me that improving venous outflow and improving CSF drainage make more sense than trying to increase the pressure of the inflow. Of course this is assumes that there is adequate inflow pressure.
Finally, high blood pressure should be corrected by the usual methods, such as exercise, smoking cessation, medications and weight reduction. We do not advocate hypertension as a treatment of MS.
DrS
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re: DrSclafani answers some questions
Hi Doc,
Have a nice vacation! (mine is finished after Sunday )
)
rgds,
Robert
Have a nice vacation! (mine is finished after Sunday
rgds,
Robert
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: DrSclafani answers some questions
Today I treated a 38 year old North American woman who consulted with me about pelvic congestion syndrome recently diagnosed by CT angiogram, done in an emergency department because of pelvic pain, that showed a dilated ovarian vein opacifying a venous plethora in the pelvis.
I share this case because this patient's medical history resembles that of a prior patient, whose pelvic congestion was treated endovascularly while neglecting to stent a renal vein compression. The result was a variety of symptoms that I often see in patients with Multiple Sclerosis, such as fatigue, heat intolerance, cognitive impairment, imbalance. These symptoms completely resolved with stenting of the renal vein. It was ultimately determined that the patient did not have MS. I thought it important to have discovered someone without MS who clearly developed classic ccsvi symptoms after occluding the ovarian vein by forcing all that renal venous blood into the vertebral plexus.
Now I have another patient with similar presentation, again without a diagnosis of MS. Today's patient complains of chronic fatigue, short term memory loss, tinnitus, left flank and back pain, tightness and spasm, heat intolerance, tinnitus, headaches, hematuria, nocturia, hesitancy and frequency and recently nausea. Sound familiar?
In the upright position, gravity tends to force blood up from the ovary using a series of valves that have one way flow toward the heart. The pelvic congestion syndrome results when blood is unimpeded in flowing downward into the pelvis. This occurs when the valve that normally allow one way flow toward the heart become incompetent. The resulting venous engorgement is associated with symptoms such as urinary blood or protein, pelvic pain, hemorrhoids, and fatigue. The recommended treatment is to block blood from descending into the pelvis by occluding the ovarian vein at its connecctions to other major pelvic veins.
The first step in treatment is to assess venous incompetency, determine anatomy and look for cause.
I performed left renal and ovarian venography and IVUS. This is best approached from the right jugular vein going down through the right atrium into the left renal vein. However, because of my suspicion of CCSVI, I chose to access the venous circulation through the right saphenofemoral junction. A bit of a challenge.
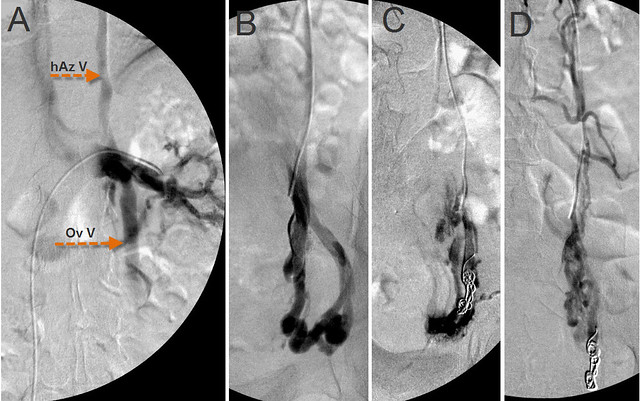
Figure 1 Treatment of Nutcracker Syndrome and pelvic congestion syndrome.
The catheter tip is in the distal renal vein. Venography (A) revealed obstruction of the left renal vein, reflux of the ovarian vein (Ov V) into the pelvis and reflux of the renal vein through the hemiazygo-renal anastomosis (hAz V) into intervertebral veins and the vertebral plexus.The renal vein contrast is markedly diminished where it is compressed by the aorta.
When a good catheter position was achieved, I used coiling and sclerotherapy to occlude proximally and distally, the incompetent ovarian vein at its pelvic anastomoses . (Figure 1 C&D) Sclerosis by sotradecol injures the endothelium and results in thrombosis.
After each step in this procedure, check venograms were performed. Control venograms were performed after each stage

Figure 2. Nutcracker treatment
A. Pre-treatment venogram. For comparison, the pretreatment venogram (A) ishows significant reflux into hemiazygous (hAzV) and ovarian vein (Ov V). After completion of the embolization and sclerotherapy of the ovarian vein (B), one now fails to see any contrast media refluxing into the ovarian vein. However reflux into the spinal Figure 2B shows that ovarian vein treatment has been successful.. No ovarian reflux is seen. However there is reflux up the hemiazygous vein. The left renal vein flow is great, With loss of the ovarian vein as a decompressing outflow, that flow must now find new routes The likely one is the hemiazygous vein,which impacts the thoracic and spinal venous drainage.
To avoid this collateral pathway, the most reasonable approach is to improve direct renal venous outflow into the inferior vena cava. After deployment of two nickel/titanium self expanding stents, one sees no contrast flowing toward the spine; it is only see flowing directly into the IVC and the right atrium.
Because her symptom complex presented a picture similar to many patients with CCSVI, I performed supine and upright Duplex ultrasound by standard CCSVI protocol. This fufilled two criteria of CCSVI, namely supine and erect reflux and long, thickened immobile valves in the left Internal jugular vein
The patient agreed to undergo venography of the left internal jugular vein at the completion of the renal vein stenting.
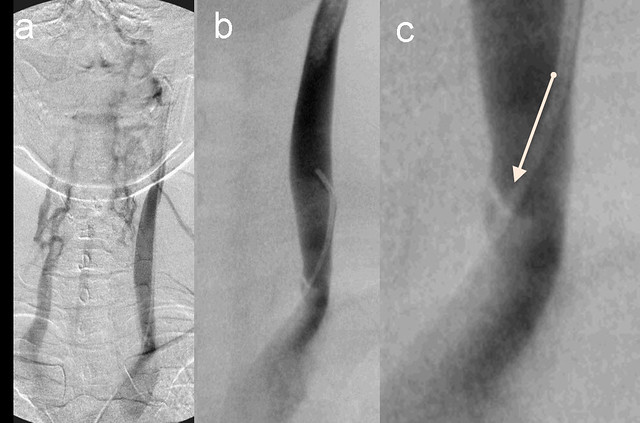
Figure 3. Internal Jugular vein valvular stenosis and reflux.
A. Left IJ Venogram showed reflux into condylar emissary , posterior cervical veins and contralaterl vertebral vein.
B. Lower jugular segment venogram shows stenosis of greater than 80 %stenosis. T
C. The zoom view shows an immobile medial valve (arrow)
This patient's medical history resembles that of a prior patient, whose pelvic congestion was treated endovascularly without stenting a renal vein compression. The result was a variety of symptoms that I often see in patients with Multiple Sclerosis, such as fatigue, heat intolerance, cognitive impairment, imbalance. These symptoms completely resolved with stenting of the renal vein. That patient did not have MS.
Today's patient complains of chronic fatigue, short term memory loss, tinnitus, left flank and back pain, tightness and spasm, Lower extremity swelling, stiff muscles and purple feet, heat intolerance, tinnitus, headaches, hematuria, nocturia, hesitancy and frequency and recently nausea. These are many of the symptoms that are commonly seen in MS and among those symptoms that are relieved by improvement in venous outflow obstructions. It is encouraging to note that the constant purple color of her feet and the tense heaviness of her legs are no longer present.. Of course, it is too soon to draw conclusions .
She is not a simple case. Rare disease is her middle name right now. She was diagnosed several years ago at Cleveland Clinic with postural orthostatic tachycardia syndrome, In addition she has mitral prolapse with mitral insufficiency as did her grandfather. In CCSVI . i am always focused on mitral prolapse in MS, thinking of Ehlers Danlos Syndrome. She does have early shoulder arthritis and many orthopedic injuries, prominent secondary palpebral fissures, easy bruisability, I think she needs to be tested. Further many of these symptoms are present in patients with MS. She needs to visit a neurologist as well.
This may very well be another case of CCSVI in a patient without MS. As such cases accumulate, evidence will mount that CCSVI is its own entity. Improvement of her symptoms may allow us to define symptoms that are specific to CCSVI.
I share this case because this patient's medical history resembles that of a prior patient, whose pelvic congestion was treated endovascularly while neglecting to stent a renal vein compression. The result was a variety of symptoms that I often see in patients with Multiple Sclerosis, such as fatigue, heat intolerance, cognitive impairment, imbalance. These symptoms completely resolved with stenting of the renal vein. It was ultimately determined that the patient did not have MS. I thought it important to have discovered someone without MS who clearly developed classic ccsvi symptoms after occluding the ovarian vein by forcing all that renal venous blood into the vertebral plexus.
Now I have another patient with similar presentation, again without a diagnosis of MS. Today's patient complains of chronic fatigue, short term memory loss, tinnitus, left flank and back pain, tightness and spasm, heat intolerance, tinnitus, headaches, hematuria, nocturia, hesitancy and frequency and recently nausea. Sound familiar?
In the upright position, gravity tends to force blood up from the ovary using a series of valves that have one way flow toward the heart. The pelvic congestion syndrome results when blood is unimpeded in flowing downward into the pelvis. This occurs when the valve that normally allow one way flow toward the heart become incompetent. The resulting venous engorgement is associated with symptoms such as urinary blood or protein, pelvic pain, hemorrhoids, and fatigue. The recommended treatment is to block blood from descending into the pelvis by occluding the ovarian vein at its connecctions to other major pelvic veins.
The first step in treatment is to assess venous incompetency, determine anatomy and look for cause.
I performed left renal and ovarian venography and IVUS. This is best approached from the right jugular vein going down through the right atrium into the left renal vein. However, because of my suspicion of CCSVI, I chose to access the venous circulation through the right saphenofemoral junction. A bit of a challenge.
Figure 1 Treatment of Nutcracker Syndrome and pelvic congestion syndrome.
The catheter tip is in the distal renal vein. Venography (A) revealed obstruction of the left renal vein, reflux of the ovarian vein (Ov V) into the pelvis and reflux of the renal vein through the hemiazygo-renal anastomosis (hAz V) into intervertebral veins and the vertebral plexus.The renal vein contrast is markedly diminished where it is compressed by the aorta.
When a good catheter position was achieved, I used coiling and sclerotherapy to occlude proximally and distally, the incompetent ovarian vein at its pelvic anastomoses . (Figure 1 C&D) Sclerosis by sotradecol injures the endothelium and results in thrombosis.
After each step in this procedure, check venograms were performed. Control venograms were performed after each stage
Figure 2. Nutcracker treatment
A. Pre-treatment venogram. For comparison, the pretreatment venogram (A) ishows significant reflux into hemiazygous (hAzV) and ovarian vein (Ov V). After completion of the embolization and sclerotherapy of the ovarian vein (B), one now fails to see any contrast media refluxing into the ovarian vein. However reflux into the spinal Figure 2B shows that ovarian vein treatment has been successful.. No ovarian reflux is seen. However there is reflux up the hemiazygous vein. The left renal vein flow is great, With loss of the ovarian vein as a decompressing outflow, that flow must now find new routes The likely one is the hemiazygous vein,which impacts the thoracic and spinal venous drainage.
To avoid this collateral pathway, the most reasonable approach is to improve direct renal venous outflow into the inferior vena cava. After deployment of two nickel/titanium self expanding stents, one sees no contrast flowing toward the spine; it is only see flowing directly into the IVC and the right atrium.
Because her symptom complex presented a picture similar to many patients with CCSVI, I performed supine and upright Duplex ultrasound by standard CCSVI protocol. This fufilled two criteria of CCSVI, namely supine and erect reflux and long, thickened immobile valves in the left Internal jugular vein
The patient agreed to undergo venography of the left internal jugular vein at the completion of the renal vein stenting.
Figure 3. Internal Jugular vein valvular stenosis and reflux.
A. Left IJ Venogram showed reflux into condylar emissary , posterior cervical veins and contralaterl vertebral vein.
B. Lower jugular segment venogram shows stenosis of greater than 80 %stenosis. T
C. The zoom view shows an immobile medial valve (arrow)
This patient's medical history resembles that of a prior patient, whose pelvic congestion was treated endovascularly without stenting a renal vein compression. The result was a variety of symptoms that I often see in patients with Multiple Sclerosis, such as fatigue, heat intolerance, cognitive impairment, imbalance. These symptoms completely resolved with stenting of the renal vein. That patient did not have MS.
Today's patient complains of chronic fatigue, short term memory loss, tinnitus, left flank and back pain, tightness and spasm, Lower extremity swelling, stiff muscles and purple feet, heat intolerance, tinnitus, headaches, hematuria, nocturia, hesitancy and frequency and recently nausea. These are many of the symptoms that are commonly seen in MS and among those symptoms that are relieved by improvement in venous outflow obstructions. It is encouraging to note that the constant purple color of her feet and the tense heaviness of her legs are no longer present.. Of course, it is too soon to draw conclusions .
She is not a simple case. Rare disease is her middle name right now. She was diagnosed several years ago at Cleveland Clinic with postural orthostatic tachycardia syndrome, In addition she has mitral prolapse with mitral insufficiency as did her grandfather. In CCSVI . i am always focused on mitral prolapse in MS, thinking of Ehlers Danlos Syndrome. She does have early shoulder arthritis and many orthopedic injuries, prominent secondary palpebral fissures, easy bruisability, I think she needs to be tested. Further many of these symptoms are present in patients with MS. She needs to visit a neurologist as well.
This may very well be another case of CCSVI in a patient without MS. As such cases accumulate, evidence will mount that CCSVI is its own entity. Improvement of her symptoms may allow us to define symptoms that are specific to CCSVI.
Salvatore JA Sclafani MD
Patient contact: ccsviliberation@gmail.com
Patient contact: ccsviliberation@gmail.com
Re: DrSclafani answers some questions
Altered flow in the VV's again, rapid symptom relief again, which would account for symptoms more logically than veins used mostly in the supine position?
We seem to have come in a circle with the questions about the importance of VV's and veins used most commonly by Upright Species.
I hear Dr Schelling is preparing a paper with his insights on the CCSVI symptoms and PTA outcomes, should be interesting hearing his experiences.
I think from memory Dr Flanagan another long time studier of this has some insights regarding flows of the VV's and 'Upright' Veins as well in his publications.
Might be a new focus coming.
Regards,
Nigel
We seem to have come in a circle with the questions about the importance of VV's and veins used most commonly by Upright Species.
I hear Dr Schelling is preparing a paper with his insights on the CCSVI symptoms and PTA outcomes, should be interesting hearing his experiences.
I think from memory Dr Flanagan another long time studier of this has some insights regarding flows of the VV's and 'Upright' Veins as well in his publications.
Might be a new focus coming.
Regards,
Nigel
Re: DrSclafani answers some questions
Maybe MS is just one form of CCSVI, except it is particularly handicapping because the blood refluxes directly into the CNS. In my opinion getting diagnosed with MS by a neurologist is the kiss of death. Better to seek a CCSVI diagnosis so one can get treatment.(PS Thanks for the great photo of the ancient Egyptian birthing clinic plaque -re Semmelweis reflex) MS Cure Enigmas.net
Re: DrSclafani answers some questions
Will you publish or present on these cases of CCSVI in patients without MS? Your conclusions seem important.drsclafani wrote:This may very well be another case of CCSVI in a patient without MS. As such cases accumulate, evidence will mount that CCSVI is its own entity. Improvement of her symptoms may allow us to define symptoms that are specific to CCSVI.
-
- Similar Topics
- Replies
- Views
- Last post