Many patients with CCSVI associated with multiple sclerosis complain of chronic fatigue. Indeed, many carry a diagnosis of chronic fatigue before they are finally diagnosed with multiple sclerosis. I became interested in chronic fatigue both from my dealings with patients with MS as well as with patients who have Nutcracker syndrome, ie, compression obstruction of the left renal vein. In fact, Nutcracker syndrome has been stated to be the most common cause of chronic fatigue in children.
Recently, I consulted with a 69 year old man who has had a diagnosis of chronic fatigue syndrome for the past 35 years. He has various medical complaints but seemed generally in good health for his age. His chief complaints besides his fatigue were memory loss, predominanly short term in nature, inability to complete his thoughts, numbness in his legs and hands, and a generalized weakness that he could not clarify as fatigue or weakness. His exam revealed a thin healthy looking man, looking younger than his stated age. On exam, he had memory disturbance, weakness in the left hip, decrease sensation to vibration and sharp touch. He weaved during his Rhomberg test and stated that his balance was bad when he walked in the dark.
He received a Doppler ultrasound in Barrie, and this was interpreted as having B-mode abnormalities and reflux on the left side.
I agreed to perform catheterization, venography and intravascular ultrasound.
the IVUS did not show the usual thickening of the valvular tissue seen in PwMS, although there were slight focal areas of echogenicity. I will not show any images.
RIGHT INTERNAL JUGULAR VENOGRAPHY
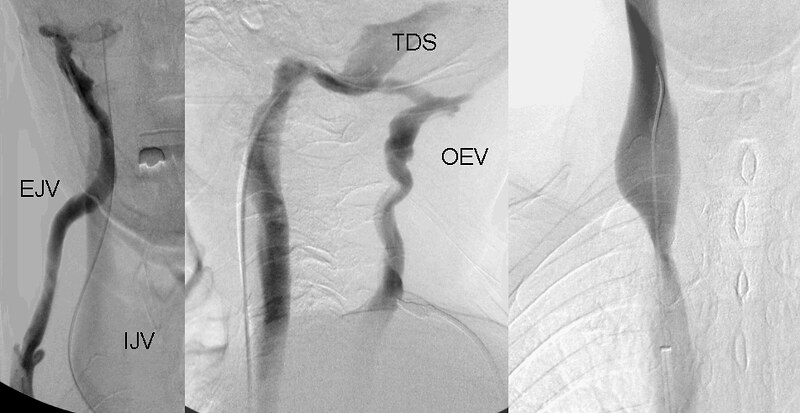
The venography of his right internal jugular vein was significant for several points.
1. The J2 segment was markedly dilated.
2. The J1 segment was markedly narrowed at the area of the inferior jugular bulb
3. There was tremendous reflux into the largest occiciptal emissary (OEV) vein draining into the external jugular vein.(EJV)
Treatment was performed with a 16mm then 20 mm high pressure balloon with moderate improvement.
The really unusual findings were seen on the left jugular venography.
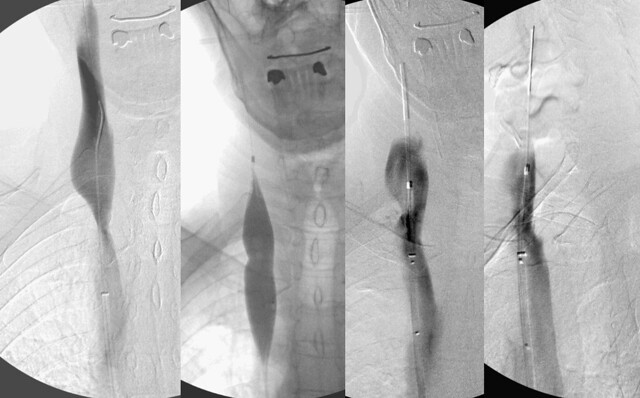
LEFT IJV venogram
The image on the left shows the inability to catheterize the left internal jugular vein beyond this stump of a vessel. This is the appearance of a completely closed valve. perhaps there is a bit of reflux through the valve just above the stump. After about 30 minutes of trying, i performed a rendevous procedure.
For those unfamiliar with this procedure, the goal is to connect the vein above the obstruction with the vein below it. In the second from left image you can see a sheath extending down the jugular but not quite reaching the catheter that had been placed from the femoral approach. In the third image you can see the wife extending down from the neck beyond the obstruction into the chest. A snare was used to grab the femoral catheter and pull it up through the obstructed valve. After this it was possible to perform the angioplasty you see.
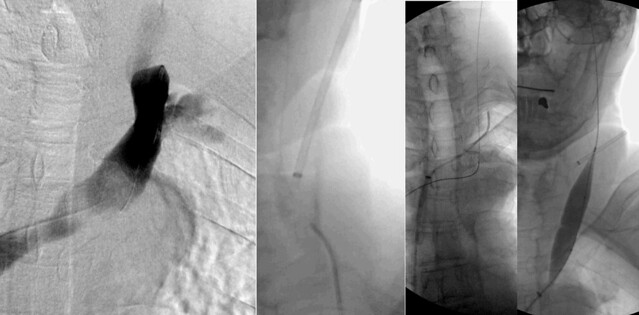
This second image of the left jugular system shows more problems, however.

The fourth and fifth images from left in the top row shows that there is clearly obstruction of the left IJV with stasis above the valve and only a trickle getting down into the chest.
On the lower row, we can see that there is narrowing of the junction of the sigmoid sinus and the internal jugular vein (image on right lower panel shows it better) There is also reflux from the left transverse sinus into the right transverse sinus which ultimately drained into the right internal jugular vein.
In essence this vein is severely obstructed in two locations at the skull base and at the inferior jugular bulb.
There can be no treatment of the lesion at the skull base. angioplasty is not feasible there.
if one looks at the upper left panel of this image one sees something else, a stenosis of the brachiocephalic vein just before it enters the superior vena cava.
This final images shows that better
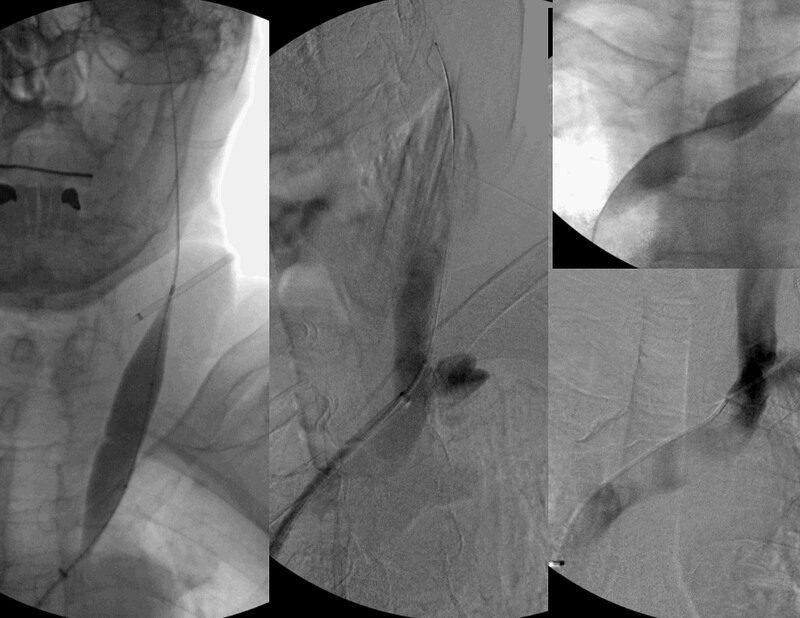
The two images in the right panel clearly show the obstructive nature of the stenosis. The waist in the balloon was eliminated with about 12 atmospheres of pressure. Such stenosis are usually caused by compression against the left brachiocephalic artery that is tortuous at this age. Is this significant? I think so. Will this angioplasty persist? I doubt it because of the compressive nature of the lesion. However the patient and I agreed to no stents on this visit.
So, he does not have MS proven, his neurologists have excluded this diagnosis. He has chronic fatigue and very severe venous outflow obstructions. I look forward to the followup in this patient because it is of importance to see whether angioplasty can improve his chronic fatigue
