Time for another interesting case report. This one illustrates the usual values of IVUS for determining balloon size, but also the value of IVUS in a case of post treatment stenosis. An interesting case indeed.
This is a 55 year old Canadian woman with SPMS who underwent treatment of both internal jugular vein stenoses in October 2010. The proceduralist detected "mild to moderate stenosis in the midportion and mild to moderate stenosis in the base of the left internal jugular vein", which were treated by 10 mm and 12 mm balloons respectively; he also detected "moderate to severe" stenosis at the base of the right internal jugular vein which was treated by "14 mm high pressure angioplasty for two minutes". They detected no azygos stenosis and did not evaluate the left renal or the ascending lumbar veins.
The patient reported "real and significant improvements" after the procedure but they were "short lived". She states that she sees "more rapid decline now" especially with balance strength and spasticity.
RIGHT JUGULAR ANGIOGRAPHY
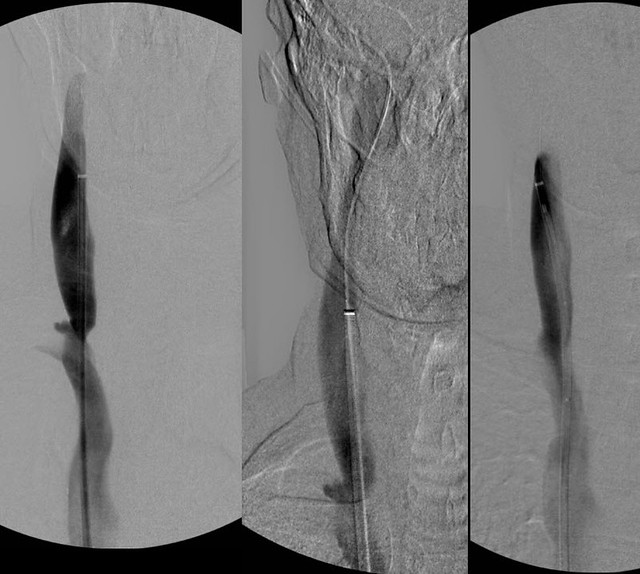
Venography (left image) of the right internal jugular vein showed a stenosis of the inferior jugular bulb. IVUS (not shown) revealed that the stenosis was the result of an immobile valve apparatus. The vein was measured such that balloon size was difficult to select. 16 mm seemed a bit too little and 18 mm seemed a bit to big. So i started with the 16 mm balloon. Venography (middle image) looked pretty good but I repeated IVUS and the valve was shown to still have some immobility and stenosis. The 18 mm balloon was used aand it was just fine with no injury and with excellent expansion of the valvular stenosis. A second followup IVUS showed a wide open valve. and the third venogram (right).
So this illustrates the venography was inadequate to size the balloon on the first treatment but IVUS was pretty accurate. IVUS also helped show that the valve was incompletely opened on the 1 mm angioplasty.
LEFT INTERNAL JUGULAR VEIN
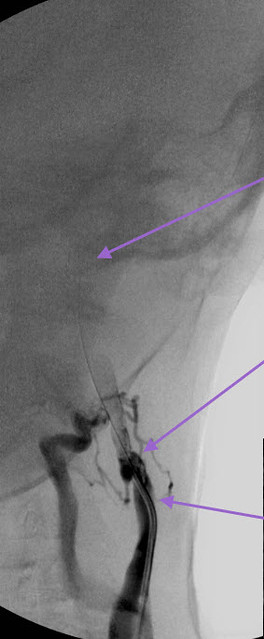
This first image (ignore arrows) illustrated the difficulties in advancing the catheter into the dural sinuses. First there were large collateral veins and the wire kept going into them. My partner thought that the jugular vein was occluded at first but with a firm injection at the site of no advancement, i could get some xray contrast media up into the upper vein. Although I could get the 14/1000th inch guidewire up, the catheter would not follow it. It was impossible to do.
So I attempted to advance the IVUS over the guidewire across this obstruction and that was successful. Then I could see the condition of the obstructed vein and the patency of the dural sinus and upper jugular.
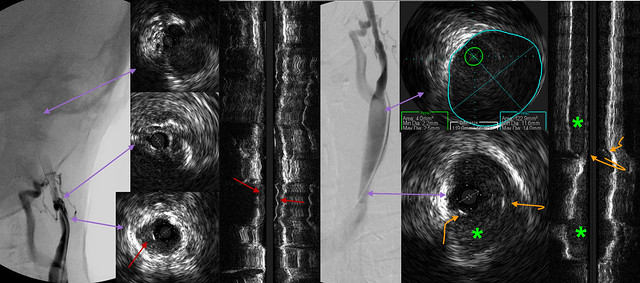
in this image the purple arrows point to corresponding sites in the ivus and the venogram. The upper upper IVUS shows that IJV was a decent size, not the largest but certainly acceptable. The middle IVUS shows the area were the catheter would not traverse. The venogram shows a tortuous area and the IVUS shows a pin hole stenosis. The lower IVUS shows that much of this narrowing may be a hypoplasia but the stenosis is made much worse by what looks like intimal hyperplasia. (red arrows).
The three right images show a venogram, and two views of the IVUS The lowest part of the venogram shows a stenosis the upper area of the venogram shows a pretty normal looking lower jugular vein in J2. IVUS shows that there is some intimal hyperplasia (green asterisks) as well as a stenosis caused by bridging tissue, possibly valve remnant, possibly adhesions (orange curved arrows)
None of this could be seen by the venogram.
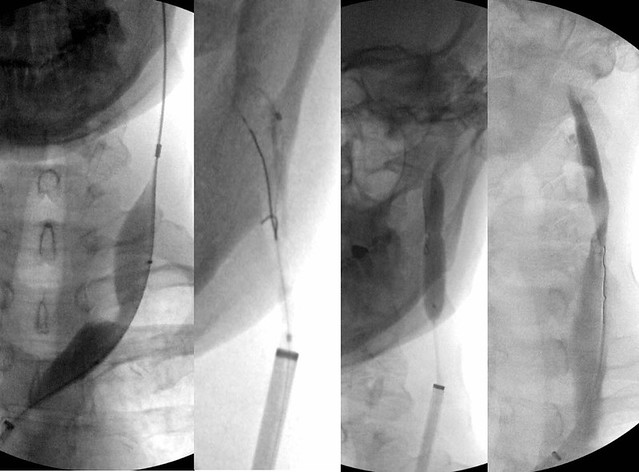
This image shows the angioplasties. First i decided to dilate the lower segment which required a 16 mm balloon. in other words, the lower obstruction required a larger balloon that had been chosed based upon venography during the patient's prior treatment. I decided to treat this stenosis first because I wanted to be able to get my sheath into the jugular vein. This might allow more forward pressure on the catheter and guidewire and allow me to get a stiffer wire across the higher stenosis. I was correct and it allowed me to force that guidewire through the upper obstruction and ultimately get the higher balloon in position. The upper stenosis required an 8 mm balloon or a smaller balloon that had been chosen based upon venography the last time.
I think that the upper stenosis may have been caused by the larger balloon angioplasty performed the first time. The IVUS and venographic appearance of the stenosis is suggestive of a thrombosis that has developed because of overdilatation. I think that this some of this clot dissolved and resulted in a recanalization track through the thrombus rather than a "mild to moderate" stenosis seen by the first proceduralist. The IVUS appearance has also influenced my decision to treat this patient with prolonged anticoagulation and antiplatelet therapy rather than my standard regimen of one month of pradaxa plus aspirin.
IVUS is the clear winner in this case.
