Hi my name is Jason & I've been diagnosed with R.R.M.S 10 days ago..
I Walk with a limp, after walking short distances my left leg feels so heavy that I have to concentrate not to trip on my foot.
I get double vision , I slur my words and I have no balance just as if I was drunk.
When i have to use the washroom . I really have to use the washroom .
I've Been Watching Video's on Youtube on my free time of this ohh soo wonderful disease I've been blessed with.
On the 3rd of May I go back to c my Neurologist
How does it work? Do I choose what Med's to start taking or does the Neurologist choose for me Suiting my Situation.
If I have a choice what do do u guys recommend and why?
I've seen a lot of video's and with every drug i hear good and bad .
Any info is good info
Feel free to reply please and thank you
Treatment options
-
centenarian100
- Family Elder
- Posts: 504
- Joined: Mon Apr 15, 2013 9:51 am
Re: Treatment options
Sorry about your diagnosis Jason. Dealing with MS is overwhelming at first, you will become a lot more knowledgeable over time and much more comfortable making decisions about your health.JTX wrote:Hi my name is Jason & I've been diagnosed with R.R.M.S 10 days ago..
I Walk with a limp, after walking short distances my left leg feels so heavy that I have to concentrate not to trip on my foot.
I get double vision , I slur my words and I have no balance just as if I was drunk.
When i have to use the washroom . I really have to use the washroom .
I've Been Watching Video's on Youtube on my free time of this ohh soo wonderful disease I've been blessed with.
On the 3rd of May I go back to c my Neurologist
How does it work? Do I choose what Med's to start taking or does the Neurologist choose for me Suiting my Situation.
If I have a choice what do do u guys recommend and why?
I've seen a lot of video's and with every drug i hear good and bad .
Any info is good info
Feel free to reply please and thank you
You can check out the national MS society for some basic information: http://www.nationalmssociety.org/index.aspx
The section on treatments is here: http://www.nationalmssociety.org/about- ... index.aspx
There are 10 FDA approved disease modifying agents for multiple sclerosis:
Aubagio (teriflunomide)
Avonex (interferon beta-1a)
Betaseron (interferon beta-1b)
Copaxone (glatiramer acetate)
Extavia (interferon beta-1b)
Gilenya (fingolimod)
Novantrone (mitoxantrone)
Rebif (interferon beta-1a)
Tecfidera (dimethyl fumarate)
Tysabri (natalizumab)
Most neurologists will treat all patients with clinically definite multiple sclerosis with an FDA approved medication.
Neurologists have different styles of practice, so I can't tell you what your neurologist will recommend, but it is a good idea to have some knowledge about anything you are putting in your body regardless of whether you made the decision about treatment or not. You are taking the risk, not your doctor. You may choose to refuse any treatment for any reason.
The most common medications used for newly diagnosed multiple sclerosis are the injectable medications copaxone, extavia, rebif, and avonex.
copaxone is a once a day subcutaneous injection
extavia, rebif, and avonex are injectable [beta-interferon] medications which have common side effects of muscle aches/fatigue/flu like symptoms/depression which are very common after the injections, especially during the first few months. Avonex is a once a week intramuscular injection which some people like.
These 4 medications have all been shown to reduce the frequency of multiple sclerosis attacks/relapses/exacerbations by about 30% in clinical trials.
tecfidera and aubagio are newly approved oral medications.
click the links on the site to learn more information
Best of luck
-Centenarian
Re: Treatment options
Thank you so much
Do you think tysabri would be good to start off with?
I Don't like the idea of a needle every day
Do you think tysabri would be good to start off with?
I Don't like the idea of a needle every day
-
centenarian100
- Family Elder
- Posts: 504
- Joined: Mon Apr 15, 2013 9:51 am
Re: Treatment options
I don't think I'm qualified to make any specific recommendation especially given that I don't know you or enough details about your specific situation.
tysabri is generally considered to be a "second line" multiple sclerosis treatment. In other words, it is usually reserved for patient's doing poorly on "first line" therapy or who have highly aggressive disease.
The reason for this is that tysabri prevents leukocyte trafficking into the central nervous system and is associated with an otherwise rare central nervous system infection called progressive multifocal leukoencephalopathy (PML).
an example of an MRI brain in an MS patient with PML (T2 FLAIR sequence):

PML can cause worsening neurological disability or death. It is caused by a virus known as JC virus which is very prevalent but does not cause significant disease in most people with a healthy immune system. PML is also a concern in organ transplant patients, AIDS patients, or other patients on immunosuppressive drugs
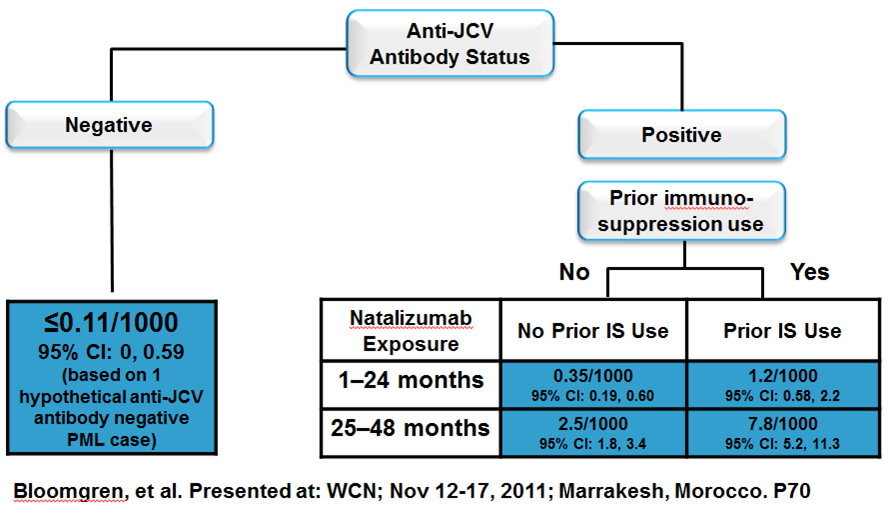
The risk of PML is dependent on the presence or absence of prior exposure to JC virus (inferred from a serum JC virus antibody test), length of tysabri use (increased risk with greater length of use), and other immunosuppressive agent exposure.
Some FDA information about PML and tysabri can be found here: http://www.fda.gov/drugs/drugsafety/ucm252045.htm
tysabri is generally considered to be a "second line" multiple sclerosis treatment. In other words, it is usually reserved for patient's doing poorly on "first line" therapy or who have highly aggressive disease.
The reason for this is that tysabri prevents leukocyte trafficking into the central nervous system and is associated with an otherwise rare central nervous system infection called progressive multifocal leukoencephalopathy (PML).
an example of an MRI brain in an MS patient with PML (T2 FLAIR sequence):
PML can cause worsening neurological disability or death. It is caused by a virus known as JC virus which is very prevalent but does not cause significant disease in most people with a healthy immune system. PML is also a concern in organ transplant patients, AIDS patients, or other patients on immunosuppressive drugs
The risk of PML is dependent on the presence or absence of prior exposure to JC virus (inferred from a serum JC virus antibody test), length of tysabri use (increased risk with greater length of use), and other immunosuppressive agent exposure.
Some FDA information about PML and tysabri can be found here: http://www.fda.gov/drugs/drugsafety/ucm252045.htm
-
MarkLavelle
- Family Elder
- Posts: 178
- Joined: Sat Dec 17, 2011 8:08 pm
- Location: San Francisco Bay area
- Contact:
Re: Treatment options
As noted, different neuros have completely different approaches, from dictator to "whatever!"JTX wrote:How does it work? Do I choose what Med's to start taking or does the Neurologist choose for me Suiting my Situation.
Better neuros will help you understand the differences and also make a recommendation, especially if your personal situation points to a particular med being best. In my case, for example, my neuro strongly recommended Copaxone because my immune system is already proven less than perfect and then compromised (cancer, chemo & radiation in the '90s). Copaxone apparently has the smallest effect on the immune system...
Best of luck!
RRMS dx 3/3/11; Copaxone since 12/1/11
-
- Similar Topics
- Replies
- Views
- Last post