NZer1 wrote:These are conclusions from hard science and have to be respected and used when it comes to actions regarding
the CRAB drugs."
Ashton Embry makes the following statement in the link that you posted: "3) The CRAB drugs do not have any effect on MS disease progression."
While it is true that copaxone has failed to meet the sustained disability endpoint in many studies, the beta-interferons have met this endpoint time and time again. Here is some data from the trials....


source: 1. PRISMS Study Group. Randomized double-blind placebo-controlled study of interferon β-1a in relapsing/remitting multiple sclerosis. Lancet 1998; 352: 1498-1504.
glatiramer acetate decreases the risk of progression to MS after CIS:
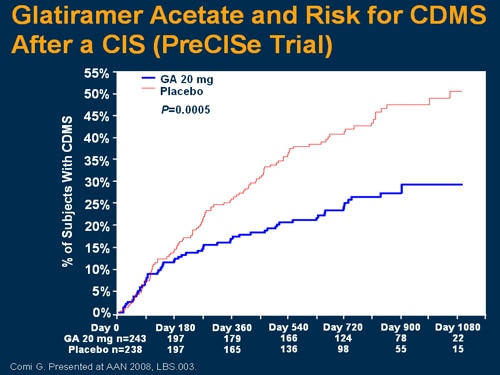
source: "PreCISe" trial
How about the new drugs?
BG12 easily met confirmed disability...

as did tysabri...

My point is that with the exception of copaxone, there is level 1a evidence (multiple randomized blinded prospective clinical trials) favoring that MS drugs do have benefit in preventing progression of disability. There is currently no high quality evidence for the disability benefit of the liberation procedure.
With regards to presumed benefit on disability progression, Dr. Embry states that "...it is mainly based on the clinical trials which tested the effect of the drugs using frequency of MS relapse and number of new MS lesions as proxies for determining if a given drug affected progression or not"
As I have shown above, it is not based on assumptions or proxies but rather is based on actually doing EDSS measurements on blinded patients. Whether or not these modest benefits are worth the enormous cost of the drugs is a different debate, and I agree with Dr. Embry's statements such as the following:
“widespread embracing of dubious and poorly validated outcomes by some MS investigators, often in contexts where there are egregious conflicts of interest, threaten academic credibility not to mention long term professional autonomy.”
However, when he is criticizing CRAB drugs and stating that they don't do anything to prevent disability progression, he is going against several high quality and well designed studies.

