Page 2 of 3
Posted: Tue Aug 23, 2011 8:27 am
by Cece
You would want the d-dimer test before the procedure to have a baseline measurement. After the procedure, it should be able to tell if there is active clotting somewhere in the body. It would not be able to find an old clot however. I think this test might be most useful in the first month after the procedure, since clots are most likely early on. It would be especially useful if the doctor does not prescribe anticlotting medication, on which there is still not a consensus.
Kate, come back and post when you can, we are all pulling for you.
Dr S on vacation
Posted: Tue Aug 23, 2011 1:27 pm
by Kate_PghPA
well it seems my local Vas. surg AND Dr S. on vacation now...
perhaps I've got my answer-- no rush for ReTreatment now...
some things ARE out of our control...
thank you all for being SO SUPPORTIVE...sincerely!
oh, and today I got a Denial letter from insurer re: Acute Inpatient hospitalization--They say should have been " Observational level'... that landed me from Independent Gait to Walker-using
--60 days to appeal...any help on This topic also much appreciated!
And we felt That 5.9 earthquake today...oi !

'rains it pours'
thanks, K.
Posted: Wed Aug 24, 2011 4:15 am
by bluesky63
Greetings from the epicenter of the earthquake.
I am so, so sorry to hear of your troubles. If your flow was decent earlier this year, who knows what is going on now? There is so much to unravel.
I also had a dramatic downturn several months after angio, and thought the worst. The good news is that I recovered *so much better* than anyone would have expected. It wasn't perfect, but it happened, and if you had asked in the spring it would have seemed impossible. I dearly would have loved a window into my body during the acute issues and after. What was going wrong? Where? How did recovery happen?
There are so many systems that interconnect, and so many different theories of what is going on when a person has an MS flare-up. If you did have a positive d-dimer, it does not even necessarily indicate a blood clot. Interestingly, many people with MS have a high d-dimer during flare-ups (this has been discussed here but I can't find it right this minute -- Marie had great info on it). I am going to try to get some links for you. I have had a very high-d-dimer during flare-ups, but no clots on chest x-rays. However, no one has scanned other areas in the past. Could there have been clotting elsewhere?
I hope this doesn't sound cold or analytical when you are having such a personal crisis. Believe me, my heart is with you. I know those dark places, and I am sending you warmth and light and hope for the best recovery.

Bottom line -- I believe that I recovered so well because my vascular system was better able to handle the event I had, whatever caused it. I deeply hope the same will be true for you, and for other people.
t.c. to Pittsburgh 'liberator'
Posted: Wed Aug 24, 2011 2:19 pm
by Kate_PghPA
t.c. to Pittsburgh 'liberator'
no call back after calling Fri. Aug. 19, t.c. again today explained situation ...no return call...

Dr. may be at a loss as to what to do, if anything
== actually doubt if I'm clotted: Plavix, ASA...may be neuro. flare up AND
ortho??? bad back after 30+yrs. of nursing...
thanks everyone...
Posted: Wed Aug 24, 2011 2:49 pm
by dania
Kate,even if you are fully anticoagulated you can still get a clot. This is part of an email I got from a doctor.
QUOTE
"The total block can be caused by clots even if anticoagulated. I recently attended a patient after his second unsuccessful attempt in the USA where they said the same non mentioning the possibility of thrombosis but scarring. They couldn't open the vein and we could in the first time, after stenting and an INR of 4.9 the stent thrombosed and we had to perform a very complex procedure with a mix of approaches and bloodthinners with final good result."
Usually doctors like to have your INR between 2.5 and 3.0 to prevent clotting. And that patient got a clot with an INR of 4.7. Doctors worry with that high INR patients could bleed and possibly causing death.
Posted: Thu Aug 25, 2011 9:37 am
by mtf
That's my case, Dania.
Could you, please, tell me more of what that Docter did to that person?
Posted: Thu Aug 25, 2011 9:52 am
by dania
mtf wrote:That's my case, Dania.
Could you, please, tell me more of what that Docter did to that person?
It is written there. He told me the patient was there for 4 weeks.
"They couldn't open the vein and we could in the first time, after stenting and an INR of 4.9 the stent thrombosed and we had to perform a very complex procedure with a mix of approaches and bloodthinners with final good results. Otherwise if the problem is not clot related but excess of scarring (restenosis) we need to pass the obstruction and use a medicated balloon."
He thinks he can do the same for me.
Posted: Thu Aug 25, 2011 10:34 am
by mtf
Thank you Dania
But, can you tell what were the complex procedure and the name of the Doc.?
Posted: Thu Aug 25, 2011 10:37 am
by Cece
An INR of 4.9 is really high. I looked up warfarin overdose:
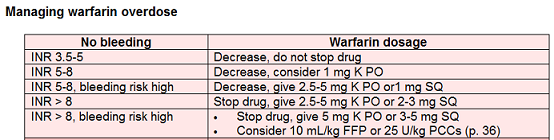 http://peir.path.uab.edu/coag/article_221.shtml
http://peir.path.uab.edu/coag/article_221.shtml
This was for INRs of that level in the absence of bleeding, there were different instructions if minor or major bleeding was present.
I would guess the category change at 5 is why the INR was 4.9 exactly?
Warfarin is an anticoagulant, not a clot-dissolving drug. I would think they'd have to use a clot-dissolving drug too. I can see why US doctors would not want to go to these extreme lengths, if the potential risk to the patient increases and could be fatal and the benefit is still not proven.
Is this better or worse than grafting, in terms of risk? Or in terms of possibility of success? I hate these 'rock and a hard place' choices.
Re: Dr S on vacation
Posted: Thu Aug 25, 2011 10:51 am
by Cece
Kate_PghPA wrote:well it seems my local Vas. surg AND Dr S. on vacation now...
perhaps I've got my answer-- no rush for ReTreatment now...
some things ARE out of our control...
How are you doing with the walking? Any recovery?
I have to say, in your situation, I would be in a rush for retreatment! We are all different. And I don't know if that would be right or not. Rushing in general can affect decision-making. I also had a very good experience with my second procedure, which brought more benefits than the first one did, and I'm now 6 weeks after the second procedure and still doing well.
Posted: Thu Aug 25, 2011 11:09 am
by mtf
Good for you Cece and all the others that are doing well.
That's not my case and many others. I think we have to find the best we can do when things aren't going well for us.
Posted: Thu Aug 25, 2011 11:19 am
by Cece
Absolutely, mtf.
We all have different degrees of MS and different types of CCSVI too, and the doctors are using different methods, so the results are different too. And sometimes there is just good luck or bad luck thrown in the mix. And doctor's CCSVI experience or inexperience.
Posted: Thu Aug 25, 2011 11:19 am
by dania
I'm with you MTF. Too many of us are joining that group .And not by choice!
I would like to be in the other group.
Posted: Thu Aug 25, 2011 11:24 am
by mtf
I would like to be in the other group too...but I'll keep trying! And so all the others (people in the bad group).
update
Posted: Mon Aug 29, 2011 6:04 am
by Kate_PghPA
confirmed: my 'liberator' MD IS out of the Country until Sept. 6
am trying to get D-dimmer test / Ultrasound ordered
what timing...GOD help me, please!
thank you all for your input