Page 2 of 4
Posted: Mon Oct 19, 2009 5:52 pm
by radeck
Just a quick first update, will post pictures when I get to it and write more when I think of it.
The MRA revealed bilateral collapses of jugular veins just above the collar bones. He suggests that this be looked at more closely with venograpy, also to see if the valves there are a factor.
Since I saw the images and how symmetric the collapses were on both sides I've been thinking about what could cause this phenomenon. On this forum we've talked a lot about the possibility that the obstructions are congenital, and somehow this seems a more likely explanation to me if it is unilateral (as I think in most of Zamboni's patients, who had more commonly left sided stenosis), but both veins being narrowed at the same height seems to be quite a coincidence. I'm wondering about the possibility that there may just not much blood running through these veins to begin with, and this sucks them squished like a cheap garden hose (borrowing this term from somebody else who first coined it). I suppose collaterals could suggest that there IS enough blood there, and needs to be re-routed. But then I've never seen the collaterals in a healthy control, so don't know if the ones I have are not normal.
Although we believe that iron deposits and hypoxia are more important, I was nevertheless happy to see that there were no new lesions.
More later.
Posted: Mon Oct 19, 2009 7:12 pm
by Rokkit
radeck wrote:I'm wondering about the possibility that there may just not much blood running through these veins to begin with, and this sucks them squished like a cheap garden hose (borrowing this term from somebody else who first coined it). I'm wondering what evidence we have against this hypothesis.
I think when Dr Dake measures the decrease in pressure gradient across the stenosis following stent placement, that's what proves there's plenty of blood wanting to go that route.
I'm glad you got some answers. Are you doing the venography and stuff and when?
Posted: Mon Oct 19, 2009 7:27 pm
by radeck
Rokkit wrote:I think when Dr Dake measures the decrease in pressure gradient across the stenosis following stent placement, that's what proves there's plenty of blood wanting to go that route.
This is very interesting. I had heard about this. If anybody can point me to more information about e.g. how the pressure gradients are measured and how large they are pre and post treatment, that would be much appreciated!
Rokkit wrote:I'm glad you got some answers. Are you doing the venography and stuff and when?
I'm glad too. It feels good to see something actually wrong in my body, as opposed to pure hypotheses. I will have venography in the next couple of weeks, to find ot what's causing the stenosis,in particular to look at the valve.
Posted: Tue Oct 20, 2009 7:02 am
by radeck
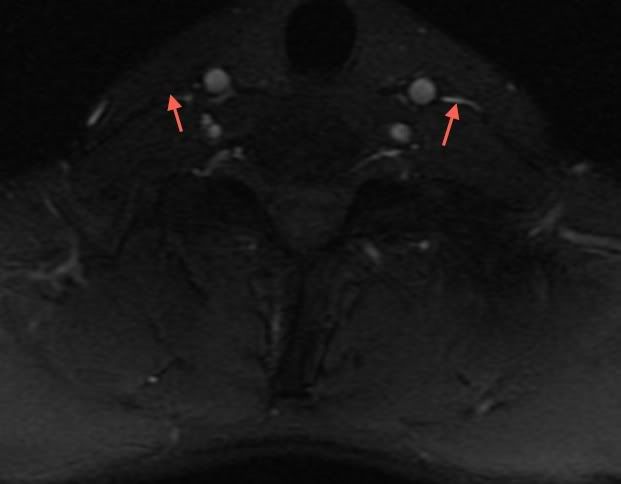
Here are two images. Red arrows point at the IJV's at height just above the collar bone, where I indicated the jugulars with red arrows.
It looks to me from the second picture like there's some pretty tough tissue (muscle?) squeezing in that jugular. So either the vein muscles aren't strong enough to hold up, and/or there's too little pressure inside the vein to act against that external pressure. The reason for that could be a too strong valve just above, or (this is me speculating) just general lack of flow because of some problem higher up (in the brain?).

Posted: Tue Oct 20, 2009 9:29 am
by mrhodes40
The pressure difference across the stenosis in me during surgery dropped by 3-4 points. It is measure in cm H2O--not the same as a blood pressure. There should not really be much pressure at all...
In one of Zamboni's papers--must have been Dec '08 cause that is where he did venograms--they also noted about a 3 point drop.
I'll find it and reference it...
Collaterals should be invisible on a regular person, what happens is tiny veins nearby are forced to stretch and take the load that can't get through the blocked area, that only happens if there is enough pressure to force it to happen, so the idea of collapsed veins that are because of not enough blood flow does not make sense to me, if that were true collaterals would not form.
back in a sec.........
edit: they use cm H2O for measurement no mmhg in this
Posted: Tue Oct 20, 2009 9:34 am
by mrhodes40
Venous pressure Pressures measured in patients and controls respectively were not significantly different (Mann–Whitney) (superior vena cava 13 (SD 4) vs 13 (4), azygous 16 (7) vs 14 (4), IJVs 14 (4) vs 12 (5)). In contrast, the pressure gradient measured in CDMS across the stenosies was significantly different. For instance, pressure in the stenotic proximal azygous vein was 3.9 cm/H2O higher as compared with the pressure measured in the adjacent superior vena cava of the same subjects (p<0.01; Mann–Whitney); equally, pressure in the stenotic IJVs was 1.8 cm/H2O higher with respect to the cava (p<0.04; Mann–Whitney
So about 4 points difference just as mine was in surgery, and this WAS from the Dec '08 paper
marie
Posted: Tue Oct 20, 2009 9:54 am
by fernando
Rad,
Your images are amazing. I can't believe how clearly one can see the stenosis.
Fernando
Posted: Tue Oct 20, 2009 10:17 am
by Arcee
In case it helps, mine was a mean across the stenosis of 2 mmHg.
Posted: Wed Oct 21, 2009 10:04 am
by magoo
Radeck, my stenosis was symmetric too. I hope you are doing well.
Posted: Thu Oct 22, 2009 5:19 pm
by bluesky63
I can understand how it would feel to know for sure that there is something physically wrong in the structure of your body that you can measure on a medical test.
Those are really amazing images. Thank you for posting them and for writing all about what you're going through. I am hoping for everything to turn out great!
Posted: Sun Nov 22, 2009 8:20 am
by radeck
My diagnostic venography appointment is tomorrow at noon. My low jugular vein collapses seemed significant on the MRV, and he wanted to find out what causes this collapse (e.g. a problem with valves), and if the problem is "dynamic". I don't know if this means he might try balloon angioplasty already tomorrow.
This has actually been my biggest confusion in all this, and even more so after watching last nights documentary about Zamboni: why does Z have success with the simple balloon widening, and only half of his patients re-stenose after two years, while D claims to find that the veins of each one of his patients immediately re-collapsed? It can't simply be a low number statistic thing: when I spoke to D in August he had treated ~40 patients, it must be quite a bit more by now - and Z has treated over a hundred. Given that Z's patients do quite well at least until a narrowing comes back, and that I only had a CIS 11 months ago, have no disability, and am stable now, ballooning seems to be the most appropriate treatment, if any treatment will be required.
Posted: Sun Nov 22, 2009 8:27 am
by ozarkcanoer
Great picture !! OK, from left to right, who is who ??
ozark
Posted: Sun Nov 22, 2009 8:29 am
by radeck
redundant post
Posted: Sun Nov 22, 2009 8:41 am
by turbotaguy
Congrats. This may have been covered in other threads (I just found this topic and am reading threads like a mad man), but did insurance cover any of this for any of you guys? If not, what was / is the approximate cost for the diagnosis and stent work?
I'm near Detroit and am looking into what is happening here and in Buffalo, but I'm always up for a trip to CA!
Posted: Sun Nov 22, 2009 8:48 am
by radeck