Page 376 of 557
Posted: Wed Aug 10, 2011 5:24 am
by drsclafani
MaggieMae wrote:drsclafani wrote:pklittle wrote:
Cases are not being scheduled???
It is odd. The perception of my availability,or my ability to treat remains confused. I can schedule but cannot manufacture patients.
Dr. Scalfani,
Could this be an issue of insurance coverage? Are patients still be covering by their insurance for this procedure or are these companies refusing (as I have read) to approve?
The only one that is not cooperative is blue cross blue shield
So far all others continue to reimburse for this procedure
Posted: Wed Aug 10, 2011 6:00 am
by pklittle
pkLittle wrote:
2. "after 30-40 minutes, I could not enter the right jugular vein. "
How do you try for that long to enter? Do you try different methods of entry?
probe and contrast
microwire probing
stiff glidewire probing
berenestein
headhunter catheter
neck ultrasound
then go and curse in the corner
then try again
Hence the benefit of the very long sheath, to avoid damage outside the area of focus, correct?
Am I learning, or what?

Posted: Wed Aug 10, 2011 6:37 am
by HappyPoet
Regarding collateral veins, here's a bit of information that might help...
Drs. Zamboni and Galeotti in Phlebology, 2010, "The chronic cerebrospinal venous insufficiency syndrome"
The main collateral pathways activated in the course of CCSVI are the condylar venous system, the pterygoid plexus and the thyroid veins. Additionally, the suboccipital cavernous sinus and the hemiazygous-lumbar venous anastomosis with the left renal vein may also become prominent substitute circles.
<
shortened url>
Posted: Wed Aug 10, 2011 7:19 am
by Cece
Can a port be removed? Does the vein heal?
My immediate reaction is anger and dismay that something that was an attempt to help a patient's MS (getting a port put in for chemotherapy) turns out to have been the wrong thing to do, since it was a jugular port. And this means the vein has been subject to toxic chemotherapy? On IVUS, can you tell if it looks scarred from this? The valve was unusually thick, could the chemotherapy have worsened it? In chemotherapy, are there any guidelines for checking to see if both jugulars are viable before inserting ports into either of them? Should there be such guidelines?

These veins are important and they have been treated as if they are not and put at risk.
Posted: Wed Aug 10, 2011 7:50 am
by HappyPoet
Cece, those are fantastic questions. We don't know where the port was implanted, but perhaps we can assume it was in the R-IJV and not the subclavian vein, for instance. Since the valve was found closed now, just think of the consequences if the valve was closed three and four years ago, too, when the chemo would have refluxed through the veins of the brain. Both IJVs, especially the valves, need to be checked before putting a port into one.
Posted: Wed Aug 10, 2011 8:18 am
by Cece
Chemo refluxing through the veins of the brain...terrible thought.
This is the post that led me to think that the port is in the LIJV. There is that puff of contrast, the unexplained slow flow in the LIJV, and Dr. Sclafani enigmaticly saying, "any port in the storm"....
www.thisisms.com/ftopicp-173178.html#173178
Posted: Wed Aug 10, 2011 8:57 am
by HappyPoet
My brain is starting to hurt.
Cece, you're a very good sleuth. Assuming a L-IJV port, could it be that he used that port to access the R-IJV valve from below the valve, and in classic rendezvous fashion, accessed the R-IJV valve from above the valve using an arm vein access site, for example? Assuming a R-IJV port, could it be that he used that port to access the R-IJV valve from above the valve, and in classic rendezvous fashion, accessed the R-IJV valve from below the valve using a Saphenous vein access site?
Did any of that make any sense at all?
Edited for punctuation and clarity.
Posted: Wed Aug 10, 2011 3:43 pm
by evangelia
Well, we have tortured veins for centuries.
Everytime we needed some kind of vessel procedure, we would use a vein . Veins were handy. Arteries were noble and always protected.
This is the revenge of the veins.
I think the port in the vein is the key .
Posted: Wed Aug 10, 2011 4:10 pm
by Cece
drsclafani wrote:pkLittle wrote:2. "after 30-40 minutes, I could not enter the right jugular vein. "
How do you try for that long to enter? Do you try different methods of entry?
probe and contrast
microwire probing
stiff glidewire probing
berenestein
headhunter catheter
neck ultrasound
then go and curse in the corner
then try again
An essential step!

Posted: Wed Aug 10, 2011 4:27 pm
by Cece
drsclafani wrote:
Venography looked like this:
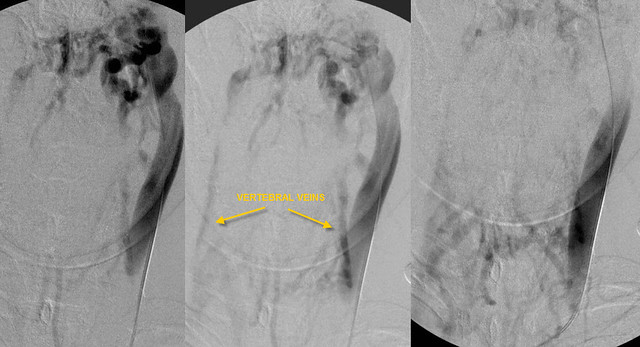
cece
if the outflow of the right internal jugular vein were obstructed, one would not necessarily visualize the right jugular vein through collaterals. Yes, this could also be an obstruction of the outflow from the transverse sinus but there are collaterals in the neck crossing the midline and one would expect some flow into the jugular.
interesting, isnt it?
Yes, very interesting, as always. This is a lot of collateral flow. It's extreme.
So the collaterals would add some flow into the right jugular unless it is blocked lower down to such an extent that the others are better, including the right EJV which is a crazy vein to be serving as a collateral route for the LIJV.
And we already know it is severely blocked lower down to the extent that you were not able to catheterize it.
When can we expect part 2?
Posted: Wed Aug 10, 2011 4:29 pm
by Cece
evangelia wrote:Well, we have tortured veins for centuries.
Everytime we needed some kind of vessel procedure, we would use a vein . Veins were handy. Arteries were noble and always protected.
This is the revenge of the veins.
I think the port in the vein is the key .
Revenge of the veins! A frightening thought.
Everything is always clearer in retrospect.
Welcome to the thread, evangelia.
Posted: Wed Aug 10, 2011 4:30 pm
by MikeInFlorida
Hi, mike....how is our mutual friend doing
Very well. Fatigue level has been lower than normal on 4 of the past 5 days. Step improvement in balance in unassisted standing posture is unabated. And oddly, the right foot is consistently the same color as the left foot (at least, very odd for her). A careful diary is being kept, and so far, all good things!
Posted: Wed Aug 10, 2011 5:58 pm
by HappyPoet
Hi Pam (pklittle),
Great job! Well done for immediately zeroing in on the importance of the port! Tell Doug that he owes you a dinner at your favorite restaurant.
Hope to see you participating on more cases!

~~~~~~~~~~
Hi MikeInFl,
Welcome to TIMS! Your "thousands of questions" made me smile. I hope your friend does well after her procedure. Lots of supine rest (so the jugulars can have extra sheer-stress time for healing) and lots of water (so important). Cheerleader (Joan Beal) has an excellent endothelial health program at the CCSVI Alliance website,
www.ccsvi.org
Hope to see you participating on more cases!
~~~~~~~~~~
Hi evangelia,
Welcome to TIMS! "This is the revenge of the veins" is, as Cece said, a frightening thought. "Revenge of the Veins" could be the name of a 1950s "B" horror movie of the kind shown at double-features at the drive-ins.
Hope to see you participating on more cases!
Posted: Wed Aug 10, 2011 6:15 pm
by newlywed4ever
drsclafani wrote:MaggieMae wrote:drsclafani wrote:
It is odd. The perception of my availability,or my ability to treat remains confused. I can schedule but cannot manufacture patients.
Dr. Scalfani,
Could this be an issue of insurance coverage? Are patients still be covering by their insurance for this procedure or are these companies refusing (as I have read) to approve?
The only one that is not cooperative is blue cross blue shield
So far all others continue to reimburse for this procedure
I can't help but wonder if Empire NY (as the middle man for other states' BCBS) is denying predetermination based on their own policy rather than individual state's; i.e. My BCBS/Michigan rep stated NY Empire considers the procedure experimental but Michigan does not.
Posted: Wed Aug 10, 2011 8:23 pm
by drsclafani
Cece wrote:Can a port be removed? Does the vein heal?
My immediate reaction is anger and dismay that something that was an attempt to help a patient's MS (getting a port put in for chemotherapy) turns out to have been the wrong thing to do, since it was a jugular port. And this means the vein has been subject to toxic chemotherapy? On IVUS, can you tell if it looks scarred from this? The valve was unusually thick, could the chemotherapy have worsened it? In chemotherapy, are there any guidelines for checking to see if both jugulars are viable before inserting ports into either of them? Should there be such guidelines?
These veins are important and they have been treated as if they are not and put at risk.
The port was placedd into the subclavian vein, not the jugular vein. I suspect that the subclavian vein stenosis resulted from puncture of the subclavian vein. The catheter tip was like located at the inominate vein and the chemotherapy might have made this stenosis.
We need a little understanding. That a port was installed is really related to the knowledge of the vein pathology.
no one is strying to hurt the veins.