Page 381 of 557
Posted: Sat Aug 13, 2011 7:55 pm
by drsclafani
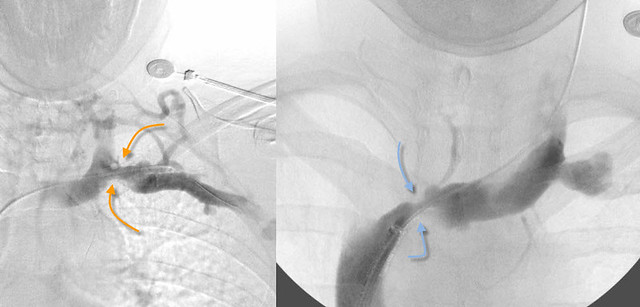
MikeInFlorida wrote:drsclafani wrote:In the gurley case reports on IJV and dural sinus thrombosis, an innominate stenosis was detected in one case (does figure 11 in the paper look familiar?

I photoshopped a quick side-by-side for ease of comparing (Gurley case on the left, Dr. S's patient on the right). Even stenosed, my wife has prettier veins.
These more closely remind me of the hurley gurley girl
Posted: Sat Aug 13, 2011 10:25 pm
by Cece
drsclafani wrote:
Now that's an innominate stenosis. You weren't kidding when you said that it's down to the size of the catheter.
Look at the collaterals in the first image coming off of the subclavian and going up. Competition between the flow from the arm and the brain...
One of the things about this case so far has been that, even though the veins are impressively bad, they're still treatable. It's better than a hypoplasia and much better than a total occlusion.
With a little worse luck, the innominate could've scarred down altogether in that focal spot and clotted together and been lost.
Posted: Sat Aug 13, 2011 10:25 pm
by Cece
drsclafani wrote:MikeInFlorida wrote:DrSclafani wrote:Both have risk but i would think that either can be managed by stents if necessary with small risk of migration. However because the stents are larger, migration is particularly "annoying"
Annoying? Wouldn't migration into the SVC (then into rt. atrium) be potentially fatal?
Mike
if you notice the quotation marks, they are there for a reason. I was intending to have poetic understatement.
You have to know me better...
lol, I suggested as much, about the quotes, but took it down so as not to be getting in the way of a discussion of the risks.

Small risk of migration is not zero risk of migration, but it becomes a matter of benefit to risk ratio.
Of course I was nervous at the the thought of a renal stent, had I turned out to have a renal stenosis, which I did not.
Posted: Sun Aug 14, 2011 2:59 am
by drsclafani
Cece wrote:drsclafani wrote:MikeInFlorida wrote:
Annoying? Wouldn't migration into the SVC (then into rt. atrium) be potentially fatal?
Mike
if you notice the quotation marks, they are there for a reason. I was intending to have poetic understatement.
You have to know me better...
lol, I suggested as much, about the quotes, but took it down so as not to be getting in the way of a discussion of the risks.
Small risk of migration is not zero risk of migration, but it becomes a matter of benefit to risk ratio.
Of course I was nervous at the the thought of a renal stent, had I turned out to have a renal stenosis, which I did not.
If you believe that the aorta and the superior mesenteric artery are really compressing the renal vein in the nutcracker syndrome (which i do), then one would realize that the renal stent would be held in place by those two structures. Moreover, the length of the left renal vein, crossing from left to right to enter the inferior vena cava, is long enough to place in most cases a 6 cm stent. the more stent, the less likely migration.
Migration is very uncommon both in jugular and in renal and iliac veins. I think the evidence is clear on that. There are other reasons to be cautious with stents but migration is not a significant issue.
Posted: Sun Aug 14, 2011 5:46 am
by MikeInFlorida
drsclafani wrote:Mike
if you notice the quotation marks, they are there for a reason. I was intending to have poetic understatement.
I think I knew that, so I don't know why I posted what I did. I apologize for that part of the post.
Posted: Sun Aug 14, 2011 8:45 am
by Cece
You had asked more than once about the risks of migration, I think you were looking for more of a discussion of it, which is valid.
Posted: Sun Aug 14, 2011 10:04 am
by Cece
drsclafani wrote:Cece wrote:
Plus there is still a whole RIJV to look at. And maybe an azygous or two. (With CCSVI, you never know....)
No pressure, Dr. Sclafani..... ;)
Maybe a little pressure.....
This case has generated a lot of interest!
patience my patient!
Still answering questions on this fascinoma
Whoever thought your patients could be patient! We are all early adopters, which lends itself to a certain educated-risk-taking, time-is-of-the-essence, impatient nature.

MS is in fact character building, even as it tears everything else down. But I've been doing really well these last several months. A lost opportunity for character building?
Posted: Sun Aug 14, 2011 2:57 pm
by NZer1
Dr. thanks for getting Frances booked.
This quote got my attention because of some reading I have done on skull changes due to fluid flows. Is the canal size something that is noticed in your work as a routine check when assessing a patients flow issues?
Quote " These images show that the transverse sinus and the sigmoid sinus had normal diameters. However there was a prominent connection between the transverse sinus inside the skull and the vertebral vein and posterior cervical branches on the outside. These vessels are connected by a very large emissary vein traversing across the skull via the hypoglossal canal. This canal is usually a very small opening in the skull but in this patient it is exceedingly large. I think this suggests that a long standing (perhaps congenital) outflow obstruction of the internal jugular vein has existed. " from page 373.
Hydrocephalus in my mind is a clue that there are forces involved because of fluid dynamics. If in CCSVI canal sizes are not normal we might be seeing a trend.
Regards all,
Nigel
Posted: Sun Aug 14, 2011 6:23 pm
by drsclafani
NZer1 wrote:Dr. thanks for getting Frances booked.
This quote got my attention because of some reading I have done on skull changes due to fluid flows. Is the canal size something that is noticed in your work as a routine check when assessing a patients flow issues?
Quote " These images show that the transverse sinus and the sigmoid sinus had normal diameters. However there was a prominent connection between the transverse sinus inside the skull and the vertebral vein and posterior cervical branches on the outside. These vessels are connected by a very large emissary vein traversing across the skull via the hypoglossal canal. This canal is usually a very small opening in the skull but in this patient it is exceedingly large. I think this suggests that a long standing (perhaps congenital) outflow obstruction of the internal jugular vein has existed. " from page 373.
Hydrocephalus in my mind is a clue that there are forces involved because of fluid dynamics. If in CCSVI canal sizes are not normal we might be seeing a trend.
Regards all,
Nigel
Nigel
i have noted very prominent emissary veins when there is severe obstructions. I thought that this was going to represent a very significant prognostic finding. Unfortuntely the sample was too small and I have noted equally obstructed outflow veins with no emissary veins.
Posted: Sun Aug 14, 2011 6:43 pm
by Cece
For anyone coming in late, here is the link for the case we are all discussing. It's eight pages back....
www.thisisms.com/ftopicp-172921.html#172921
Re: IVUS Images
Posted: Sun Aug 14, 2011 10:32 pm
by NHE
Hi Dr. Sclafani,
What is the thickness of the image slice in the IVUS cross sectional images that you post? I'm curious how much depth there is to the image.
Thanks, NHE
Posted: Mon Aug 15, 2011 1:21 am
by CureOrBust
Cece wrote:MS is in fact character building, even as it tears everything else down. ....A lost opportunity for character building?
What does not kill us, makes us stronger? too bad patience is considered a virtue...
Posted: Mon Aug 15, 2011 3:18 am
by MikeInFlorida
drsclafani wrote:If you believe that the aorta and the superior mesenteric artery are really compressing the renal vein in the nutcracker syndrome (which i do), then one would realize that the renal stent would be held in place by those two structures. Moreover, the length of the left renal vein, crossing from left to right to enter the inferior vena cava, is long enough to place in most cases a 6 cm stent. the more stent, the less likely migration.
Please clarify... to whom does this quote apply? Cece's case, the current patient's case, or is it a general statement about CCSVI pathology?
drsclafani wrote:Migration is very uncommon both in jugular and in renal and iliac veins. I think the evidence is clear on that. There are other reasons to be cautious with stents but migration is not a significant issue.
I have not heard of this evidence; it is relieving to hear that it exists. But
1. Could you provide a quick summary of the "other reasons to be cautious with stents"?
2. I believe that stents are subject to metal fatigue/fracturing. If true, does it depend on the amount of movement at the placement site (I believe you have discussed this before)?
3. Are stents available that prevent endothelialization (or whatever the correct word is that represents the endothelial cells encasing it)?
Re: IVUS Images
Posted: Mon Aug 15, 2011 3:20 am
by drsclafani
NHE wrote:Hi Dr. Sclafani,
What is the thickness of the image slice in the IVUS cross sectional images that you post? I'm curious how much depth there is to the image.
Thanks, NHE
good question.
i must admit i do not know the answer to it.
i will explore
S
Re: IVUS Images
Posted: Mon Aug 15, 2011 3:34 am
by MikeInFlorida
drsclafani wrote:NHE wrote:Hi Dr. Sclafani,
What is the thickness of the image slice in the IVUS cross sectional images that you post? I'm curious how much depth there is to the image.
Thanks, NHE
good question.
i must admit i do not know the answer to it.
i will explore
S
What does the "thickness of the image slice" mean?