Page 395 of 557
Re: DrSclafani answers some questions
Posted: Sun Oct 02, 2011 10:12 am
by Cece
AZYGOUS VEIN
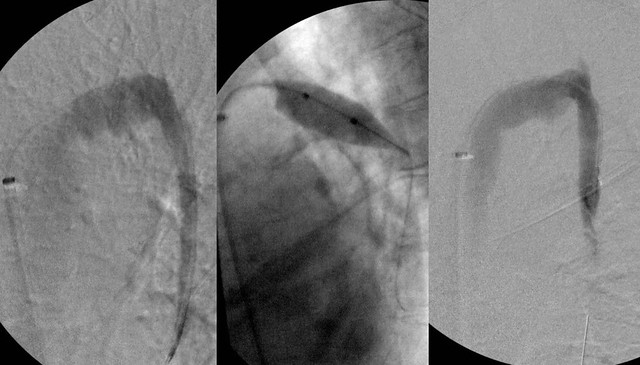
there was very high flow in the azygous vein and irregularities in the azygous arch. IVUS showed two immobile valves on the arch. A 14 mm balloon was used to 6 atmospheres with good result. IVUS showed no valve problem after treatment. But flow was very strong and the vein itself was very large, suggesting to me that we were dealing with a Nutcracker syndrome.
Yes, a 14 mm balloon in the azygous is a big vein here too....
Why though did I have a large azygous and rapid flow but no Nutcracker....my best understanding builds on what you've said before, that my verts were well developed and flow goes from the verts to the spinal veins to the azygous, and from my xl condylar veins to the spinal veins to the azygous.
Without the ivus images, I don't think it looks like there's anything wrong with the azygous arch in the first image. Do you agree?
Re: DrSclafani answers some questions
Posted: Sun Oct 02, 2011 10:16 am
by Cece
Squeakycat wrote:With women more susceptible to MS than men, I wonder if differences like this in basic anatomy play a role in that differentiation?
It's an intriguing line of thinking. But what causes the greater elasticity in the veins in men? Is it as simple as testosterone? Maybe Chaz Bono is onto something....!
Re: DrSclafani answers some questions
Posted: Sun Oct 02, 2011 10:22 am
by Cece
RENAL VEIN AND ASCENDING LUMBAR VEIN
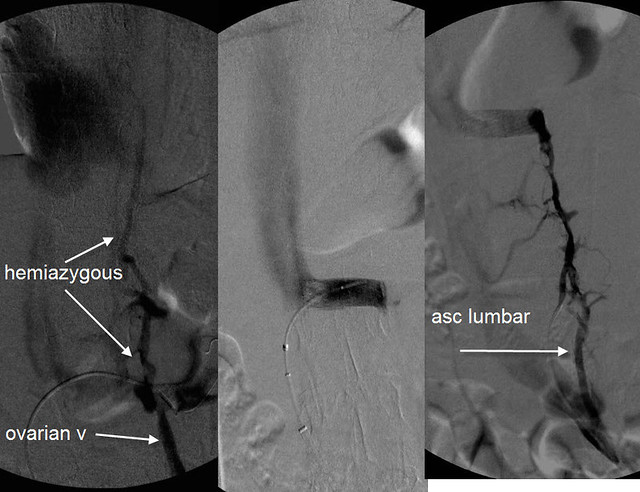
The renal venogram shows a classic Nutcracker syndrome. The contrast is "light" as the vein nears the inferior vena cava. this is caused by the compression. There is dense filling of both the ovarian vein and the hemiazygous vein which are being used as collaterals to drain the left kidney of its high blood flow volume. On the left is seen the ascending lumbar vein. this also connects to the renal vein.
I have to go now and I just got to the most interesting of the veins posted. Bluesky, we haven't heard from you, what do you think? I really appreciate seeing the hemiazygous and ovarian veins in the image and that the contrast is filling in them and what that means. I am however a doofus who is not entirely sure where the renal vein and the inferior vena cava is in the image.
edited: ok, middle image, we are seeing the renal vein with the catheter in it, and the larger light vein to the left going up must be the inferior vena cava. Were the ascending lumbars also being used as collateral veins? That's not good.
Re: DrSclafani answers some questions
Posted: Sun Oct 02, 2011 2:54 pm
by Cece
drsclafani wrote:RNutcracker syndrome may be a clinically occult problem in healthy patients but in patients with compromised outflow of the azygous vein, additional blood flow enters the vertebral plexus and the spinal veins. thus compounds the CCSVI resulting from the stenoses of the right and left IJV and the azygous vein.
But these images of the renal vein and collaterals were taken after the azygous was treated, correct? So even after the azygous was treated, it appears that there is contrast going into the ascending lumbars? By the time you got to this part of the procedure, the patient had corrected flow in the jugulars and in the azygous. It's interesting.
After the competion of the procedure the patient upon questioning volunteered information regarding chronic pain near the left ovary that was, to her reminiscent of pain in the ovary during menstruation. (she is post menopausal). Thus i believe that she has pelvic congestion caused by reflux of renal vein blood into her ovarian vein resulting from the nutcracker syndrome.
mystery solved....
It will be interesting to see whether her ovarian symptoms improve now that the renal vein has been opened. However the high flow down the ovarian vein has resulted in incompetence of the valves of her ovarian vein and she may not get relief without treatment of the ovarian vein syndromed.
The treatment is blockade of the ovarian vein from the flow in the renal vein by embolization.
Ovarian vein valves! That was helpful to explain it. High flow in the wrong direction would indeed be detrimental to the function of valves meant to control flow in the opposite direction. Embolization would seal off the vein to the incoming wrong-way flow from the renal vein, allowing things to flow the right way again, even without working valves.
whew, I worked through this case, next case please!

There was a whole month without them, you know. Such hardship.
(But no pressure, much respect for your limited time, etc!)
Re: DrSclafani answers some questions
Posted: Sun Oct 02, 2011 10:43 pm
by CureOrBust
Cece wrote:I notice you used a 15 atm balloon on the second jugular. Is it relatively rare to need to go that high? What is the highest that you are currently comfortable going?
For my right Jugular, he ended up using 20mm at 15atm after he found that an 18mm (my vein was 16mm) did not resolve a waist in the balloon. And if I am reading it right, IVUS showed that I needed a larger balloon on my left as well. 20mm at 13atm. He did note that I was on the extreme side, so I guess not common.
Re: DrSclafani answers some questions
Posted: Mon Oct 03, 2011 3:21 am
by drsclafani
Cece wrote:drsclafani wrote:
RIGHT IJV

There is a valvular stenosis at the confluens with bulging of the right sided valve cusp. 18 mm high pressure balloon used. 8 atmospheres needed to open. Results looked very good to me.
LEFT IJV

There is valvular stenosis at the confluens. Neither the cusps nor the valve leaflets were visible on venography but valve stenosis was seen on IVUS. Angioplasty with 14 mm high pressure balloon was used. Pressure was 15 Atmospheres
I would think an 18 mm balloon on one side and a 14 mm balloon on the other side means that she has large jugulars, overall. Were these large jugulars or about typical? Do you think there might be a better outcome in terms of symptom improvement in patients with a greater total jugular CSA after the procedure?
Dr. Tucker was saying in another thread that men have greater elasticity in their jugulars than women do. Would that mean that female jugulars are more prone to injury if overstretched by ballooning? It also seemed to mean that male jugulars, being elastic, would have a greater capacity as holding tanks which would mean less reflux. I wonder if anything can be done (or medication taken) as an adult to increase the elasticity of the jugulars.
I notice you used a 15 atm balloon on the second jugular. Is it relatively rare to need to go that high? What is the highest that you are currently comfortable going?
that data is currently being tabulated. As a guesstimate, I would say that pressures necessary to eliminate the waist and have negative test for elastic recoil in the jugular veins ranges from 5 Atmospheres to 26 atmospheres. the average would be somewhere around 14 atmospheres. In the azygous veins the pressure is much lower in the range of 5-8 atmospheres.
However if required pressures reach 18-20 atm successful COMPLETE angioplasty is not 100% successful.
I might add that pressure is not the only methodology. I do not go above 18 atm until after the fifth incomplete dilatation.
Tabulation should be finished in about one week.
Re: DrSclafani answers some questions
Posted: Mon Oct 03, 2011 3:23 am
by drsclafani
Cece wrote:drsclafani wrote:
RIGHT IJV
There is a valvular stenosis at the confluens with bulging of the right sided valve cusp. 18 mm high pressure balloon used. 8 atmospheres needed to open. Results looked very good to me.
LEFT IJV
There is valvular stenosis at the confluens. Neither the cusps nor the valve leaflets were visible on venography but valve stenosis was seen on IVUS. Angioplasty with 14 mm high pressure balloon was used. Pressure was 15 Atmospheres
I would think an 18 mm balloon on one side and a 14 mm balloon on the other side means that she has large jugulars, overall. Were these large jugulars or about typical? Do you think there might be a better outcome in terms of symptom improvement in patients with a greater total jugular CSA after the procedure?
This is certainly within the range. perhaps a bit larger than normal
Re: DrSclafani answers some questions
Posted: Mon Oct 03, 2011 3:29 am
by drsclafani
Cece wrote:drsclafani wrote:
RIGHT IJV
There is a valvular stenosis at the confluens with bulging of the right sided valve cusp. 18 mm high pressure balloon used. 8 atmospheres needed to open. Results looked very good to me.
LEFT IJV
There is valvular stenosis at the confluens. Neither the cusps nor the valve leaflets were visible on venography but valve stenosis was seen on IVUS. Angioplasty with 14 mm high pressure balloon was used. Pressure was 15 Atmospheres
Dr. Tucker was saying in another thread that men have greater elasticity in their jugulars than women do. Would that mean that female jugulars are more prone to injury if overstretched by ballooning? It also seemed to mean that male jugulars, being elastic, would have a greater capacity as holding tanks which would mean less reflux. I wonder if anything can be done (or medication taken) as an adult to increase the elasticity of the jugulars.
The incidence of angioplasty injury seems pretty rare these days.
Most of the original injuries during the mis-sized era seemed to have been in women but the majority of the patients are women. so not enough data to make a statement.
actually men have larger jugulars in general but the largest jugulars i have =seen have been in women.
If the vein is obstructed, then the vein tends to dilate above the stenosis. I think that collaterals are more important than stretch in relieving obstruction and reducing reflux
Re: DrSclafani answers some questions
Posted: Mon Oct 03, 2011 3:30 am
by drsclafani
Squeakycat wrote:Cece wrote:drsclafani wrote:
Dr. Tucker was saying in another thread that men have greater elasticity in their jugulars than women do. Would that mean that female jugulars are more prone to injury if overstretched by ballooning? It also seemed to mean that male jugulars, being elastic, would have a greater capacity as holding tanks which would mean less reflux. I wonder if anything can be done (or medication taken) as an adult to increase the elasticity of the jugulars.
With women more susceptible to MS than men, I wonder if differences like this in basic anatomy play a role in that differentiation?
i am skeptical that this is significant, if correct.
Re: DrSclafani answers some questions
Posted: Mon Oct 03, 2011 3:31 am
by drsclafani
Cece wrote:AZYGOUS VEIN
there was very high flow in the azygous vein and irregularities in the azygous arch. IVUS showed two immobile valves on the arch. A 14 mm balloon was used to 6 atmospheres with good result. IVUS showed no valve problem after treatment. But flow was very strong and the vein itself was very large, suggesting to me that we were dealing with a Nutcracker syndrome.
Yes, a 14 mm balloon in the azygous is a big vein here too....
Why though did I have a large azygous and rapid flow but no Nutcracker....my best understanding builds on what you've said before, that my verts were well developed and flow goes from the verts to the spinal veins to the azygous, and from my xl condylar veins to the spinal veins to the azygous.
Without the ivus images, I don't think it looks like there's anything wrong with the azygous arch in the first image. Do you agree?
This data is also being reviewed. Preliminarily: venography looks normal in 40 per cent of the azygous valvular stenoses found by IVUS
Re: DrSclafani answers some questions
Posted: Mon Oct 03, 2011 3:33 am
by drsclafani
Cece wrote:RENAL VEIN AND ASCENDING LUMBAR VEIN
The renal venogram shows a classic Nutcracker syndrome. The contrast is "light" as the vein nears the inferior vena cava. this is caused by the compression. There is dense filling of both the ovarian vein and the hemiazygous vein which are being used as collaterals to drain the left kidney of its high blood flow volume. On the left is seen the ascending lumbar vein. this also connects to the renal vein.
I have to go now and I just got to the most interesting of the veins posted. Bluesky, we haven't heard from you, what do you think? I really appreciate seeing the hemiazygous and ovarian veins in the image and that the contrast is filling in them and what that means. I am however a doofus who is not entirely sure where the renal vein and the inferior vena cava is in the image.
edited: ok, middle image, we are seeing the renal vein with the catheter in it, and the larger light vein to the left going up must be the inferior vena cava. Were the ascending lumbars also being used as collateral veins? That's not good.
in the middle image there is a stent. that is why you are not seeing the hemiazygous and the ascending lumbar vein
Re: DrSclafani answers some questions
Posted: Mon Oct 03, 2011 6:56 am
by Cece
drsclafani wrote:Cece wrote:RENAL VEIN AND ASCENDING LUMBAR VEIN
Ok, I can see the stent in the middle and last image. That is the renal vein. That means the last image is just the usual one with contrast meant to light up the ascending lumbars, which look good.
The first image, now if I follow the catheter, that must be in the renal vein where it is releasing the contrast. I wonder what vein the catheter is in to get to the renal vein and why the vein the catheter is in does not light up? But the IVC is the very light vein that goes to the left and up. And the renal is compressed by an unseen artery so its flow is diverted to the hemiazygous and ovarian veins, which is why the contrast is able to light them up. The dark cloud at the top left of the image is unimportant.
Now that I've got the layout down, wow, that is an extreme change from the first to the second image. Once the stent is in, nothing lights up but the renal vein and the IVC.
What I am taking from all of this is that, instead of pelvic congestion syndrome affecting the cerebrospinal drainage, it is the messed-up cerebrospinal drainage that has affected the pelvic veins.
Re: DrSclafani answers some questions
Posted: Mon Oct 03, 2011 6:57 am
by Cece
drsclafani wrote:Tabulation should be finished in about one week.
!! That is exciting.
Re: DrSclafani answers some questions
Posted: Mon Oct 03, 2011 7:14 am
by Cece
drsclafani wrote:This data is also being reviewed. Preliminarily: venography looks normal in 40 per cent of the azygous valvular stenoses found by IVUS
Very nice!
You've seen the abstract on IVUS presented at CIRSE, with a very small sample size but similar findings that IVUS was able to show stenoses not seen on venography?
http://www.thisisms.com/forum/chronic-c ... ml#p175921
Another side of the coin is if there are any cases that are the opposite, where venography shows an apparent stenosis that, upon using IVUS, is not a real one. And you must be tabulating how often the venography looks normal in the jugulars too but IVUS reveals a stenosis. Is this less common in the jugulars than in the azygous?
Re: DrSclafani answers some questions
Posted: Mon Oct 03, 2011 1:57 pm
by pelopidas
According to these findings, it seems that IVUS must be part of the standard procedure of a venogram. Otherwise both diagnosis and treatment are incomplete.