Page 420 of 557
Re: DrSclafani answers some questions
Posted: Sat Jan 14, 2012 7:51 pm
by drsclafani
cervocuit wrote:drsclafani wrote:cervocuit
i will bet that homo erectus had constipation, heart disease and chronic cough. The survival of the fittest left him far behind.
Jugular hypertension is usually a reflection of problems of the heart and lungs. If right heart hypertension occurs from heart failure or emphysema, that pressure will be reflected into the jugular veins. So reflux can occur if the valves are absent. The difference is that it is not a closed system as with valve stenosis.
So what happens if the jugular valves are present with heart problems. the high pressure above the heart will close the valves if if works correctly. Then we have a closed system as with valve stenosis. Are heart desease and MS associated conditions ?
I do not think that they are associated at all.
The closed circuit obstruction is quite different from the open circuit obstruction. Closed circuit obstruction requires intracranial reflux.
Right heart failure causes reflux IF the valve is incompetent but there is still flow toward the heart at some part of the cardiac cycle or the patient is dead
But the real issue is not whether CCSVI causes MS. It is whether correction of ccsvi results in improvement of symptoms
Re: DrSclafani answers some questions
Posted: Sat Jan 14, 2012 8:32 pm
by drsclafani
mo_en wrote:Hi, best wishes to all.
Dr S, i would like to bring back a question from the past that seems to have passed unanswered:
The ability of each IJVr to act as a collateral for the other depends on the patency of the confluence of sinuses between the left and right side. I've been told that underdevelopment or even absence of the confluence is commoner than one would expect. If such an obstacle was present then someone would need both her/his IJVs to remain functional in order to have adequate outflow.
Do you consider the state of the confuence of sinuses critical? Do you intend to incorporate it in your future procedures?
Thank you.
But in the majority of patients both jugular veins are obstructed, so these collaterals are not necessarily going to allow flow from one side to decompress to the other side any way.
Not all the collaterals are intracranial or contralateral, although these are certainly important. There are also ipsilateral intracranial collaterals through the emissary veins, predominantly condylar emissary veins. Other cross collaterals include facial vein to facial vein, anterior jugular to other side, thyroid collaterals to other side, then there ipsilateral collaterals such as the external jugular veins,
Re: DrSclafani answers some questions
Posted: Sat Jan 14, 2012 9:57 pm
by drsclafani
blossom wrote:dr. sclafani,
thanks for answering.
the numbness is worse and has increasingly gotten painful. this has spread across the private part and into the right leg also. i never in 20 yrs. had a symptom just pop up and then maybe lighten up like say rrms. mine were slow steady down hill ppms type. until i had the angioplasty and woke up to the numb left leg. with this spreading from the nerve getting injured "similiar to a reflex sympathetic sympathy" type condition and it were to spread more i doubt i could live with it. you as a dr. knows rsd has no cure either. i hope i'm dead wrong i'm no dr. all i know is what my body tells me and it's not good what happened. i knew going in maybe it might not help but never expected to have this outcome. i had enough going on as it was.
again i appreciate your input. and in your experience if you have heard of this happening to anyone what if anything can be done to fix it?
after 20 yrs. i can hardly move but severe pain and numbness was not an issue. i have never taken an ms med. or anything stronger than an asparin.
what a shame if this is added to this pot of misery-and all i wanted was the hope of moving again.
when doing the doppler they checked the whole left leg for flow and that was good.
difficult to advise you over the internet on this subject. Lots of testing, lots of treatments, nothing definitive in treatment
i have had one patient in whom i placed a nephrostomy in which the initial needle went through an intercostal. His pain was persistent
Re: DrSclafani answers some questions
Posted: Sun Jan 15, 2012 11:19 am
by Cece
drsclafani wrote:There are also ipsilateral intracranial collaterals through the emissary veins, predominantly condylar emissary veins.
I have been wondering about those condylar emissary veins, and whether, as you have suggested, in some patients they indicate a congenital malformation of the valves leading to increase as a fetus in the size of the emissary veins.
Here's an image from a patient after bilateral ligation of both jugulars, due to a cancer of the neck.
http://neurosurgery.dergisi.org/pdf/pdf_JTN_554.pdf

Are there condylar emissary veins in this image?
I think I'll pull another image from the article and ask about it too. Next post....
Re: DrSclafani answers some questions
Posted: Sun Jan 15, 2012 11:29 am
by Cece

What do you make of this image? It's a DSA after unilateral internal and external jugular ligation on the left side. Right jugular can be seen. I think I see a vein leaving the left sinus; do you know what vein that is? Are those cerebral veins that can be seen on the left side of the brain but not the right? Does this indicate slowed drainage of the left side of the brain, as compared to the right side?
Re: DrSclafani answers some questions
Posted: Fri Jan 20, 2012 5:31 pm
by drsclafani
Cece wrote:drsclafani wrote:There are also ipsilateral intracranial collaterals through the emissary veins, predominantly condylar emissary veins.
I have been wondering about those condylar emissary veins, and whether, as you have suggested, in some patients they indicate a congenital malformation of the valves leading to increase as a fetus in the size of the emissary veins.
Here's an image from a patient after bilateral ligation of both jugulars, due to a cancer of the neck.
http://neurosurgery.dergisi.org/pdf/pdf_JTN_554.pdf
Are there condylar emissary veins in this image?
I think I'll pull another image from the article and ask about it too. Next post....
it is very difficult to see the condylar emissary veins on the frontal venogram because they are superimposed. on the lateral veiwe the vein is seen really well. I had a case today where the IR called the condular vein the vertebral vein.
The condylar vein can drain into the vertebral vein but most of the vessels go posteriorly into the back of the neck and drain into the jugular vein or into the subclavian vein. I have noted reduction in pain in the back of the neck near the skull after angioplasty of the jugular vein.
Re: DrSclafani answers some questions
Posted: Fri Jan 20, 2012 5:34 pm
by drsclafani
Cece wrote:
What do you make of this image? It's a DSA after unilateral internal and external jugular ligation on the left side. Right jugular can be seen. I think I see a vein leaving the left sinus; do you know what vein that is? Are those cerebral veins that can be seen on the left side of the brain but not the right? Does this indicate slowed drainage of the left side of the brain, as compared to the right side?
This is the venous phase of the direct injection of the left internal carotid artery, so we are seeing drainage of the left side of the brain. So we are seeing cortical veins draining into the sinuses and then crossing over to the right jugular vein via the right and left transverse sinuses.
Re: DrSclafani answers some questions
Posted: Fri Jan 20, 2012 5:58 pm
by Cece
drsclafani wrote:This is the venous phase of the direct injection of the left internal carotid artery, so we are seeing drainage of the left side of the brain.
Ahhh...that explains it. I was reading too much into one side having veins showing and the other not.
If you're still around, any thoughts on ISET? Did Dr. Zamboni present trial results on plethysmography? Was there discussion of IVUS? Fewer cowboy accusations?
Hope you are having an excellent January. I am coming up on my one year anniversary since CCSVI treatment. Still going strong.

I had a case today where the IR called the condular vein the vertebral vein.
Must've been a big condylar vein to be mistaken for a vertebral vein.
Thank you for all that you have done and continue to do for us CCSVIers!
Re: DrSclafani answers some questions
Posted: Sat Jan 21, 2012 6:51 am
by drsclafani
Cece wrote:drsclafani wrote:This is the venous phase of the direct injection of the left internal carotid artery, so we are seeing drainage of the left side of the brain.
Ahhh...that explains it. I was reading too much into one side having veins showing and the other not.
I had a case today where the IR called the condular vein the vertebral vein.
Must've been a big condylar vein to be mistaken for a vertebral vein.
hold on, cece. i never said those veins were not condylar veins. In fact, there are probably condylar veins there. All that density at the upper neck is more likely condylar than other collaterals. it just takes a good lateral view to see it well. I used to call these collaterals going into the vertebral veins too. But since i h ave been performing dural sinography, it is clear that they are very often condylar collaterals. I will try to post one today here and on my facebook page.
If you're still around, any thoughts on ISET? Did Dr. Zamboni present trial results on plethysmography? Was there discussion of IVUS? Fewer cowboy accusations?
I did not go to Miami. I havent kept up with ISET.
Hope you are having an excellent January. I am coming up on my one year anniversary since CCSVI treatment. Still going strong.
Great! I am hoping for longer times between restenoses as i am comfortable with the IVUS-based large balloon high pressure technques. Yesterday it took eleven inflations of a 14 mm balloon at 23 atmospheres to open a stenosis. That is a new boundary!
Thank you for all that you have done and continue to do for us CCSVIers!
I would like to do more treatments.
Re: DrSclafani answers some questions
Posted: Sat Jan 21, 2012 8:02 am
by Cece
drsclafani wrote:
hold on, cece. i never said those veins were not condylar veins. In fact, there are probably condylar veins there. All that density at the upper neck is more likely condylar than other collaterals. it just takes a good lateral view to see it well. I used to call these collaterals going into the vertebral veins too. But since i h ave been performing dural sinography, it is clear that they are very often condylar collaterals. I will try to post one today here and on my facebook page.
I will google condylar too, so I am more clear on what we're discussing. There is also the distinction between the vertebral vein on both sides and the vertebral plexus veins that mixes me up sometimes.
Great! I am hoping for longer times between restenoses as i am comfortable with the IVUS-based large balloon high pressure technques. Yesterday it took eleven inflations of a 14 mm balloon at 23 atmospheres to open a stenosis. That is a new boundary!
Wow, yes, lots of inflations at a high pressure, but without taking the balloon size up to 16 or 18.
Thank you for all that you have done and continue to do for us CCSVIers!
I would like to do more treatments.
Quality not quantity....not much comfort, perhaps, but the quality is there. Did you see DougL's testimony of what you did for his girlfriend?
http://www.thisisms.com/forum/chronic-c ... ml#p185024
An azygous 100% blocked, and you were persistent and got through. A jugular surrounded by bone, that you identified, and did not balloon and cause pain. A patient who left with warm hands, bright colors, better cognition, and now better walking.
Re: DrSclafani answers some questions
Posted: Sun Jan 22, 2012 6:34 am
by drsclafani
Cece wrote:drsclafani wrote:
Great! I am hoping for longer times between restenoses as i am comfortable with the IVUS-based large balloon high pressure technques. Yesterday it took eleven inflations of a 14 mm balloon at 23 atmospheres to open a stenosis. That is a new boundary!
Wow, yes, lots of inflations at a high pressure, but without taking the balloon size up to 16 or 18.
Thank you for all that you have done and continue to do for us CCSVIers!
Cece, i do not sweat the larger size WHEN it is necessary. This particular patient had venoplasty on the right side with an 18 mm balloon. IVUS showed that anything less on the right would have been suboptimal to me.
On the other hand, IVUS showed that 14 mm was optimal on the left side and i was loath to, but tempted, to use a 16mm when ten inflations were unsuccessful. However we got lucky and dilatation was successful on the eleventh inflation
S
Re: DrSclafani answers some questions
Posted: Sun Jan 22, 2012 5:55 pm
by msfire
Hi Dr S. (saint) in regards to high pressure and large balloons, I recall you using an 18mm balloon @ 18 atmospheres on my left jugular and a 22mm @ 18 atmospheres on my right. So far so good.
Re: DrSclafani answers some questions
Posted: Sun Jan 22, 2012 8:46 pm
by drsclafani
msfire wrote:Hi Dr S. (saint) in regards to high pressure and large balloons, I recall you using an 18mm balloon @ 18 atmospheres on my left jugular and a 22mm @ 18 atmospheres on my right. So far so good.
Thanks for letting me know. Those are the largest balloons / pressures combinations I have used. IF you are whom i think you are, , you are a female making it even more astounding that such balloons were used. Is that right? Remember I do not have a patient named msfire! Would you send me an email at
ccsviliberation@gmail.com so i can learn more about how you are doing?
S
Re: DrSclafani answers some questions
Posted: Mon Jan 23, 2012 9:26 am
by Cece
drsclafani wrote:Cece, i do not sweat the larger size WHEN it is necessary. This particular patient had venoplasty on the right side with an 18 mm balloon. IVUS showed that anything less on the right would have been suboptimal to me.
On the other hand, IVUS showed that 14 mm was optimal on the left side and i was loath to, but tempted, to use a 16mm when ten inflations were unsuccessful. However we got lucky and dilatation was successful on the eleventh inflation
S
I would not have predicted success on the eleventh try!
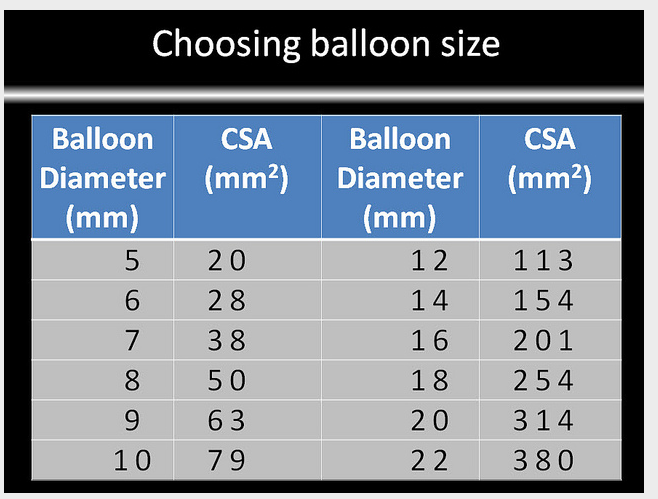
In the past we've discussed the very long inflations, and that this might cut off oxygen to the vein wall itself. So I am guessing these were eleven inflations of relatively short or medium durations, so as not to hurt the vein. A longer duration of inflation might've made for a successful dilatation in fewer inflations but at the risk of oxygen deprivation to the vein walls or even thrombus forming above the balloon during extended ballooning? What I always keep coming back to is that there is a lot to the techniques of the procedure, and that it needs to be optimized, and even then it must be proven that it is optimized, and standardized! Not an easy task.
The chart for sizing by IVUS:
But since i h ave been performing dural sinography, it is clear that they are very often condylar collaterals. I will try to post one today here and on my facebook page.
Re: DrSclafani answers some questions
Posted: Tue Jan 24, 2012 3:02 am
by MarkW
Hello Dr S,
Is it OK for me to share this chart with NICE in UK ?
Thanks
MarkW