Re: DrSclafani answers some questions
Posted: Sun Jan 06, 2013 11:25 am
I am very interested in your opinions about Dr. Rosa's study too. Any information or observations would be greatly appreciated. 
Welcome to This is MS, the leading forum for Multiple Sclerosis research and support. Join our friendly community of patients, caregivers, and researchers celebrating over 20 years of delivering hope through knowledge.
https://www.thisisms.com/forum/
Going from image 2 to image 3 is shocking! What looked like one vein was really two veins. Without the second image, it would easily be misinterpreted as a larger jugular than it was. I don't think you've shown us that before.drsclafani wrote:Left IJV
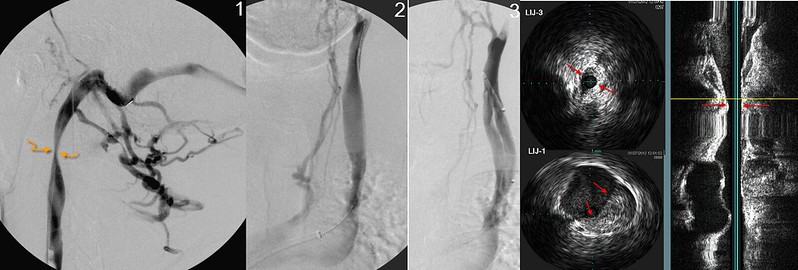
image #1 shows tremendous reflux through numerous emissary veins that drain into the posterior cervical vein. A high grade stenosis at the second cervical vertebra narrowed the vein to less than 2 mm diameter. Flexion/extension, and rotation imaging with IVUS did not show any improvement in luminal area.
image #2 showed those cervical collaterals draining slowly and also showed reflux in pharyngeal veins. A typical valvulare stenosis was seen in the lower J1 segment on both ivus and catheter venography. . I was quite surprised that the apparently large diameter of he middle of the jugular vein actually was an early division into a facial vein and the internal jugular vein. This is important if you do not perform ivus because one could easilyil oversize the balloon based on the apperently large IJV on image #2
Without performing a catheterization of the dural sinus ()image 1), the interventionalist would have missed this upper jugular lesion.
I can see it. The arrows help. Nice catch. That can't be easy.drsclafani wrote:azygos treated too.
Venography did not see a problem but ivus revealed a thickened valvular stenosis in the azygous arch
I think it's a compression and ballooning won't last. Am I wrong?drsclafani wrote:
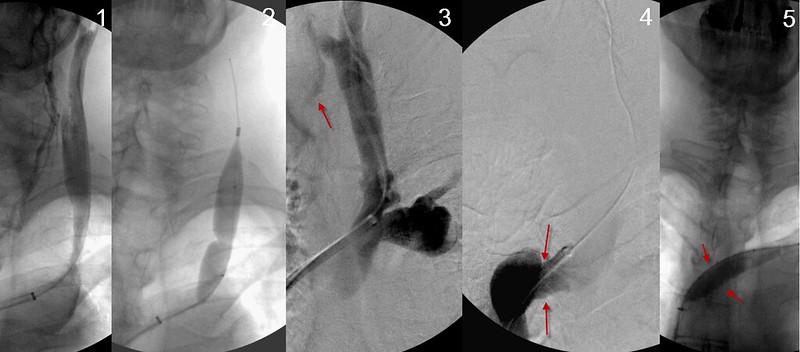
Angioplasty of the J1 segment was pretty good (see image 3). However in the same image one sees collaterals refluxing in image 3 (red arrow). Also look at the dilated subclavian vein to the right of the IJV on image 3, suggesting that there was obstruction in the brachiocephalic vein. Image 4 shows a narrowing in the brachiocephalic vein. We treated that with angioplasty too.
Ok I am trying to follow and understand this exchange. Notadoc was giving credit to the stent placement by Dr. Sclafani for fixing a C1/C2 misalignment that impinged on the jugular vein. But Dr. Sclafani is saying that in his images, the stenosis is seen at a lower level. Not the C1/C2 atlas or skull base area but down a bit at J3. No subluxation was seen but a stenosis which is usually caused by compression. I believe that means muscular compression. This area was stented and, between this and everything else that was treated, notadoc saw improvement, which is always good.drsclafani wrote:notadoc wrote:http://www.erinelster.com/files/jvsr%20 ... d%2081.pdf
I was one of the subjects in this study by Dr. Elster. I do not agree that my problems should be attributed to the disagreement I had with that horse many years ago, but I do strongly support the hypothesis that the misaligned C1/C2 was impinging on the jugular vein and contributing to the MS symptoms. Fortunately, the stent that Dr. Sclafani placed in that jugular seems to have resolved the problem so I no longer need the upper cervical treatments. That is even more fortunate because Dr. Elster has sold her practice and moved on, plus she would no longer treat me with the stent in place. I hope you will comment on the paper, Dr. S. It has been eleven months since you treated me and everything is great. Great thanks for choosing this route.
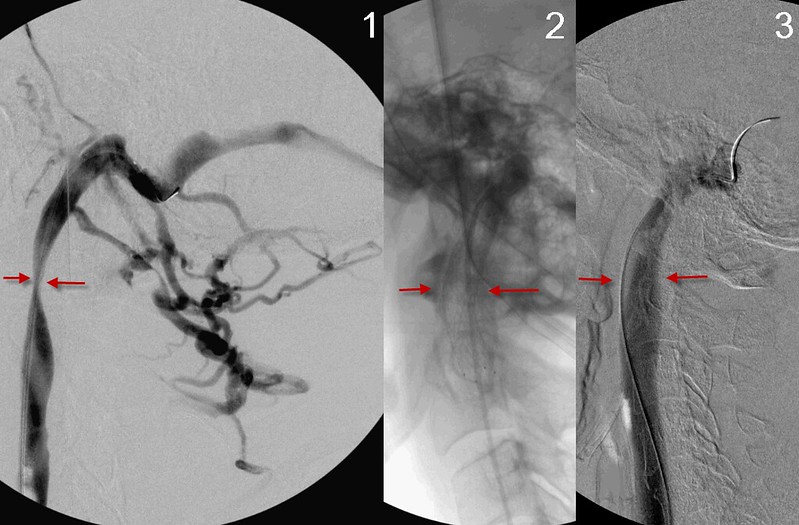
here the focus is on the J3 segment stenosis. It is not located at the skull base, but more inferiorly. I didnt recognize any subluxations on my images. This stenosis is usually caused by a compression and treatment is usually not successful. I haven't put many stents in but I have treated several patients who have had problems with stents placed by others. Problems include migration, kinking, fracture, intimal hyperplasia. I havent seen a thrombosis yet. The details are a bit murky now but i think i treated by stenting because the usual angioplasty of the valves did not result in better flow. After stent placement (see image 3) there is no reflux in the emissary veins and the stenosis is no longer present.
Blossom, i think you are mistaken about how i came to be involved in ccsvi. four women from connecticut broadcast emailed many academic vascular specialists seeking an east coast alternative to the work that Michael Dake was doing at Stanford. They sent me some transcripts of a meeting in Bologna from early 2009. I studied more than Zamboni's multiple papers before I agreed to try this procedure. There were many papers that were studied about embryology, anatomy, pathology, MRI, CT, MRV, ultrasound, catheterization, angioplasty of veins. In fact it took me months of intense study and learning to become curious and to be willing to see my first patient. Shortly after that I traveled to Toronto to hear Dr Zamboni speak. Later in the spring of 2010 I traveled to Bologna and Ferrara to further study with Salvi and Zamboni.blossom wrote:hi dr. sclafani, i hope you keep in mind that when ccsvi came about and you were starting to treat "i could be wrong" but i think dr. zambonni research was pretty new and he had done the only published paper. you were one of the first "maverick" ir's that decided to follow in the usa and treat ccsvi. it was new and i along with many appreciate your perseverance and staying with us as more is learned and more are helped.
although, chiropractics is not a new idea of treating it has been treated with prejudice by mainstream med. for a long time. so, you'll find very few published papers and peer reviewed things. but, you will find testimonials here on tims and elsewhere of it's positive effects through history. and, now with the upright mri more proof.---even dr. amir that is treating ejc's wife has no published papers but many of his patients report amazing results.
chiro.'s will never do an ir's job when venoplasty is necessary, ir's will not do any spinal adj. ir's and chiro.'s will not do dental as dr. amir is doing. and orthopedic or neurosurgeons that will come into play soon i hope will do their own thing. but, for the patients sake, getting to a place where all these things are checked out and evaluated will ultimatly bring the best results. getting this all together won't be easy for sure. but, all the above can effect blood and csf flow--not to mention nerve involvement.
the proof is in results--it may at this time, because this is new to you seem like strange bedfellows but as you explore and think out of the box as you have done with ccsvi i think it will get clearer.
It is all about expertise and point of view, Robert. I am a bit surprsed by the very strong objection to ccsvi. I think it is part ego, part finance, part corporate, part ignorance, part reaction to patient advocacy and poor politics. I dont think that you are going to get collaboration in the current environment of denial and a lack of impetusRobnl wrote:So, what is happening in Holland?? ehh..nothing!!drsclafani wrote:
I have been using the retrospectoscope and I have noted an increasing percentage of my patients are coming from Europe, including finland, denmark, germany, poland, england, scotland, ireland, italy, greece, switzerland and france.
I know that many of my patients, and presumably other Europeans, learned of me from reading on TIMS. Iam curious to hear there opinions about the state of CCSVI in Europe. What is the attitude of European neurologists regarding CCSVI? How many centers and doctors are currently operating in Europe? Is there governmenetal obstruction, interference, meddling in patient affairs? What are the reasons that patients would travel across the Atlantic to be treated in the USA? What obstacles exist to treatment in their own country? in neighboring European states? in the United States?
For those Northamericaners, similar questions: would you go back, if yes, why? if no, why not? what are the impediments? What are the benefits?
Any comments would be welcome. We North Americans always have a slanted opinion and in this international crisis, we need to understand each other
thanks
DrSclafani
First, it's forbidden by law to do medical prescanning a.k.a. scan 'healthy' persons.
Secondly, ccsvi is dismissed by neurology in Holland. Why? well, there are 2 major hospitals that are seen as the ms centers; VU amsterdam and EMC Rotterdam (there are other neuro's with ms as focus but not from 'university' point of view)
i contacted EMC in 2011, talked about ccsvi and my improvements after angioplasty...they were very happy for me, but veins are not the focus of the EMC MS research.
Now they have a study going on about fatigue and they called me to join. But my fatigue is more or less gone after treatment by dr. S. Again, they were very happy for me
VU is very drug focussed and tries to find genes and cells that could trigger the immune system, they did a small CCSVI MRI study, but did not know what they were doing. Although results were 'mixed' there was no follow up..
There were also two scanning studies done by two other hospitals....and again there were 'some' results, but no follow up.
The missing word in the studies? Expertise.
So, Holland still follows the auto immune hypothesis and attacks the immune system with drugs...
There are still some private clinics in Europe, but the treatments in hospitals are stopped, why? I spoke to one of the hospitals...they stopped not because of the FDA warning (FDA cant warn europe), but for the possible consequences of the FDA warning.
Also, treatments are mostly (except dr Simka) done without any research, only jugs and some azygos. So results are doubtful, most (except 'simple' problems) improvements fade....
Concerning te current status of CCSVI i believe the opinion of dr.S:
CCSVI is not MS, but a seperate condition with similar symptoms; the lucky ones only have ccsvi. ccsvi occurs i most of MS patients. (correct me if i'm wrong Doc)
Does ccsvi lead to ms??? i dont know, but if neurology, IR's and vascular specialists would stick their heads together maybe the progress in knowledge would go much faster.
Lets hope the results of current trials will give a boost and eyes will open.
Why did i go to New York? Because it's the most complete treatment at this moment with the most CCSVI knowledge in an objective view.
My 2 cents,
Robert
I agree Dania. I think it is well known that CSF drainage is impaired in MS. I have always suspected that rapid changes in patient condition after treatment of venous outflow obstructions by balloon angioplasty was related to rapid alterations in blood flow and CSF dynamics. Venous drainage is very important in CSF dynamics.dania wrote:With 2 angioplasties and 3 jugular vein bypasses which all produced improvements but unfortunately were short lived. I then had a Fonar upright MRI with Dr Scott Rosa (I am in his study) and Dr Damadian. It showed that my CSF flow, was not draining from my brain adequately. They also did X rays which showed my atlas was out of alignment. I improved with AO adjustments but like angioplasty they too were short lived as I cannot hold the adjustment and slip back out of alignment.So which came first in my case? Impaired CSF flow or CCSVI?
Although provocative, the findings and hypotheses of Doctor Rosa and his associates are sure to be controversial, for many of the same reasons that CCSVI shook things up. Both theories fly in the face of traditional MS dogma, and offer explanations for neurodegenerative disease that differ greatly from those proffered by mainstream neurology. Multiple Sclerosis is nothing if not complicated, and its pathogenesis is almost certainly multifactorial. It’s doubtful that any one theory will prove to be THE key to solving the entire MS puzzle, but, with research, some of these “radical” theories may have the potential to unlock some of the many mysteries held by MS. The exploration of alternative theories, done responsibly, can only benefit patients as doctors broaden their horizons. And start to think out of the box.
http://www.ncbi.nlm.nih.gov/pubmed/22733409
thanks, i pretty much agree with youEJC wrote:Now the EHC has closed shop on CCSVI I'm not sure - there's certainly nothing openly publicised.drsclafani wrote:
thanks
so strike off england and scotland from treatment options. So bizarre coming from countries that were so instrumental in the development of thoughtful approaches to surgical treatments.
Are there facilities that will do ultrasounds?
You can speak to the care providers, but as there is a such a strict hierarchy in the UK, if NICE don't approve it, it won't happen.drsclafani wrote:
Can you speak with your primary care providers about alternative treatments? Is there pressure to chastise and condemn doctors that are curious or supportive?
Currently any medical specialist that refers a patient for alternative therapies puts themselves at risk of being struck off altogether. There is little compulsion or support for medical professionals to look at alternative therapies and treatments. Some such as Osteopathy and Chiropractor are starting to become accepted. This all covers treatment offered by our National Health Service.
Of course if you're willing to pay for private treatment you can have anything you want, pretty much unrestricted. This obviously leads to a lot of problems and sorting the wheat from the chaff becomes a difficult exercise.
CCSVI in the UK has not been stopped by any governing body or threat of legal action. It's been stopped as the insurance to perform the procedure has been increased to a level that it is no longer financially viable for either the patient or the provider.
With regard to the work Dr Amir does on Emma, the important thing to understand is Dr Amir is a dental specialist that has undergone Chiropractic and Osteopath training. Ultimately he is treating Emma as a dental specialist for a TMJ and jaw problem and associated misalignment of the C1 vertebra. A side effect of this is symptoms currently attributed to MS in Emma are being eradicated.
The problems start to mount as soon as it's suggested that Jaw/skeletal misalignment treatments are treating MS.
My understanding of "MS" is it is a collection of symptoms of which the cause is currently not understood. It's a label into which you can place people for the purposes of medical categorisation. Modern drug based medicine is still pursuing the autoimmune line. If you want to anything other than that - I'm afraid you're on your own with no official support.
I would be astonished if in years to come someone finds a single cause of "MS". In fact I suggest "MS" will never be cured, what will happen is it will probably be broken down into it's component symptom parts and each patient treated for the particular problem causing their particular set of symptoms. Be that skeletal problems, vascular problems maybe along with some other issues yet to be discovered. At that point of understanding "MS" will cease to exist as each patient will have been correctly diagnosed with a specific problem causing their particualr set of symptoms.
What is criminal though is that distinct lack of publicly funded or backed research into anything other than drug based "cures".
There are some very influential interventionalists in europe who are very antagonistic about ccsvi. i have spoken with them and they are adamant that the entire idea is "snake oil". No even worthy of study. Seems like they are very influential in european IR practice acceptancegirl69 wrote:So what's happening in Switzerland ? Well, not much, at least here in the French part... The official position of the MS society aknowledges the existence of the "CCSVI phenomenon" but does not recommend testing or of course, any other action. One should remember that this is a country of pharmaceutical companies and their influence is very strong. When I first heard about Dr. Zamboni's research, I tried for months to find an open-minded IR or neuro or any doctor really. Needless to say that I didn't succeed and decided then to go to Poland, one of the first places in Europe to offer such a treatment. I always wanted to go see Dr. Sclafani though, as impressed as I was with his attitude and I always had in mind the importance of experience (I believe he was the one who said that an IR had to at least see a 100 or so cases to know what to look for...). When he had to stop treating for a while, I was so dissapointed but kept hoping that he would come back... Which he thankfully did !So yeah, I've been to NY and I would go again, because I believe that Dr. Sclafani offers the best treatment option with a constant ability to learn and improve, priceless !!!
Otherwise, I finally did find an open-minded IR here willing to do the check-ups, but although she works in quite a big clinic, I'm still the ONLY CCSVI patient she has ever seen...
Thanks for the drawing. I find it curious that patients with MS do not have hoarseness, caused by compression of the vagus nerve. Why is that? I could say the same about dr arata's blogs about the vagus nerve. Shy no hoarseness? it is the most clinically verifiable problem of the vagus nerveHappyPoet wrote:blossom, terrific post, especially about how Dr. Zamboni's work was the only published work about CCSVI when IRs started to offer venoplasty for CCSVI.blossom wrote:hi dr. sclafani, i hope you keep in mind that when ccsvi came about and you were starting to treat "i could be wrong" but i think dr. zambonni research was pretty new and he had done the only published paper. you were one of the first "maverick" ir's that decided to follow in the usa and treat ccsvi. it was new and i along with many appreciate your perseverance and staying with us as more is learned and more are helped.
although, chiropractics is not a new idea of treating it has been treated with prejudice by mainstream med. for a long time. so, you'll find very few published papers and peer reviewed things. but, you will find testimonials here on tims and elsewhere of it's positive effects through history. and, now with the upright mri more proof.---even dr. amir that is treating ejc's wife has no published papers but many of his patients report amazing results.
chiro.'s will never do an ir's job when venoplasty is necessary, ir's will not do any spinal adj. ir's and chiro.'s will not do dental as dr. amir is doing. and orthopedic or neurosurgeons that will come into play soon i hope will do their own thing. but, for the patients sake, getting to a place where all these things are checked out and evaluated will ultimatly bring the best results. getting this all together won't be easy for sure. but, all the above can effect blood and csf flow--not to mention nerve involvement.
the proof is in results--it may at this time, because this is new to you seem like strange bedfellows but as you explore and think out of the box as you have done with ccsvi i think it will get clearer.
Dr. Sclafani, by limiting your research only to peer-reviewed, published studies, you'll be missing out on a wealth of knowledge and new ideas that are included in articles and case studies.
What search terms would you like us to investigate with "upper cervical chiropractic"? Multiple sclerosis? If yes, may I ask why? Many of us believe "MS" is really just a catch-all for patients with neurological symptoms. I believe that searching by neurological symptoms, such as migraine, will give the most information.
Logically, correcting the positioning of one's misaligned Atlas makes sense to me which (for those who haven't seen it yet) is depicted by this animation:
Blue = jugular vein
Red = carotid artery
Yellow = vagus nerve
http://www.atlantotec.com/en/fundamenta ... agus-nerve
edit: included link
there are other treatments of venous ulcers associated with chronic venous insufficiency. They attempt to reduce the reflux through the saphenous vein into the leg by sclerosis or other ablating the incompetent valves of the saphenous vein. Other approaches look for May thurner syndrome, especially with left sided cvi. There are other methodologies as well. but that is not my expertise.1eye wrote:My benefits are in large part now gone, and I never got the improvements in spasticity, heat-intolerance and loss of strength in leg and fingers on my left that would have really cured me.For those Northamericaners, similar questions: would you go back, if yes, why? if no, why not? what are the impediments? What are the benefits?
I would go to see you in a heartbeat if I could drive. I also think I might benefit from endoscopic surgery on my third ventricle.
Another impediment, since October, has been an increasing infection in my left foot, now on my 4th course of longer and stronger antibiotics, with no blood testing, one set of x-rays, inconsistent care by a half-dozen or so traveling nurses, never being able to see my own doctor, nor the same doctor twice. It is a venous ulcer that started in a skin scratch, and I believe is now in the bones of my ankle (I have a history of childhood osteomyelitis). I think I have the circulation in that quadrant of my body, of someone much older, largely because of no driving. I have abandoned my wheelchair because of weakness and being able to use a walker.
Canada is in the grip of a gerrymandering election-stealing PM whose hero was Bush Jr., and would never offend big pharma. His government recently defeated legislation to speed nationwide CCSVI research, and in another bill, lower cost HIV drugs to Africa. I thought it was a different country I lived in, but I guess money can buy some things.
Is there a treatment, besides compression stockings, for CVI in legs?
Vision is a very complicated thing, with involvement of the lens, optic nerve, brainstem and occipital cortex in perception and sight. cranial nerves are responsble for accomodation and pupillary reflexes in the iris , the extraocular muscles must work in synchronization. In other words, there is no one answer to the question and a detailed explanation would far exceed my expertise. Double vision often relates to the eyes not being in sync, the eyes are out of sync.Cranial Nerves 3, 4, and 6 are responsible for d extraocular muscle movement. Pyridostigmine bromide inhibits the destruction of acetylcholine by cholinesterase and thereby permits freer transmission of nerve impulses across the neuromuscular junction movements. This may reduce the imbalance for a while and allow better vision.EJC wrote:Dr S,
I've spent the weekend thinking about the conversations on this thread and forum in general and I have a question specifically related to your understanding of the CCSVI procedure and improvements in eyesight. This is now the most debilitating symptom Emma has - double vision, poor ability to focus and eyes that at times seem to operate entirely independently of each other.
I know I've mentioned Emma's improvements before - her explanation was it was like switching from grainy old cable TV to the vibrance of HD TV at the flick of a switch.
I've read elsewhere on here that Cece also had a similar reaction.
How do you think this occurs? What is the mechanism that so instantly generates improvements?
On a related topic, my 78 year old father suffers from Myasthenia Gravis (one of the vast list of medical issues he has) for which he's prescribed Pyridostigmine tablets that pretty much deal with his issues (which interestingly are pretty similar to Emma's). He gave Emma one of tablets last week which after about a half hour straightened up her double vision and made things a whole world more comfortable. This last about 4 hours then receded - which we understand is about the operating window of that particular drug.
Any idea how this would be interacting with eyesight issues attributed to MS?
whew, thanks Cece.Cece wrote:I thought I should mention that I think it is more than okay for Dr. Sclafani not to offer advice regarding the upper cervical care ideas. It is not his discipline (interventional radiology) and it is not proven. The burden is on those practitioners (Dr. Rosa, Dr. Amir) to prove their ideas. There is a different burden on Dr. Sclafani to prove his own ideas regarding CCSVI (the use of IVUS, the impact of renal vein compression on extracranial drainage, the existence and optimal treatment of CCSVI, etc).
Registries, randomized controlled trials. Funding. Presenting at conferences. Influencing other researchers. Sharing observations.
I see too a difference between our perspective as patients and a doctor's perspective as a doctor. We are individuals. We are most concerned about our own outcome, which we may already know if we've had the procedure done, and we may be in search of alternatives if we cannot afford another procedure or there was vein injury or our symptoms did not respond to the procedure. But to a doctor, there is always a chance for a fresh start in the next patient. Always a chance to get it right. So it is okay if Dr. Sclafani focuses on what he can directly do, which is get it right in the next patient. I think he has shown through his engagement with us here that he is a remarkably caring doctor. And to whatever extent he has been able to optimize his own techniques and influence other researchers in that regard, it is of great benefit to us collectively.
A good new year to all of us.