SophieandElle wrote:Hi Dr. S,
What does it mean if your IR says that your IJV narrowing is too dangerous to mess with? Mine is right at C1. I am a bit disappointed hearing this after the test. Do you ever find them too dangerous to try to fix?
Dear Sophieandelle
sorry about that. I had answered this question but it appears never to have been transmitted. Thanks to cece for bumping it up
Of course, I cannot speak for your IR. C1 lesions are uncommon compared to lesions located at the base of the jugular vein as it enters the chest, the so-called "J-1 segment. When C1 (The J-3 segment) lesions are present they are almost always associated with lesions elsewhere, such as in the Azygos vein or in the J1 segment.
J-3 lesions are usually caused by compression between the vertebra and tendons. they are often transient, meaning that there is some expansion in certain neck positions. For example the vein might open up on internal or external rotation of the neck or by flexion and extension of the neck. Their significance is unclear because there are no papers on this area and some of my patients get clinical improvements by opening up the "fixed" stenoses in the J1 segment.
These lesions are considered challenging by some and dangerous to others. Because this is an extreminsic compression, angioplasty may have little long term impact on the narrowing, thus requiring stenting to overcome the compressive forces. Also the compressive forces are strong and may result in kinking of the stent or fracture of the stent or intimal hyperplasia. The area of stenting also contains closely proximate nerves that can result in long term pain or damage to the cranial nerves. . Finally, the J3 segment of the vein is usually much smaller than the J2 (middle part of the vein) or J1. Thus, if the stent slips out of position, it can migrate out of the jugular vein.
I find decisions about treating these J3 lesions to be very difficult. Risks are present, clinical improvements are unclear or unsubstantiated, especially when the outcomes are comfounded by treatment of other lesions.
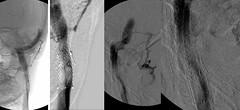
Here is an example of a normal J3

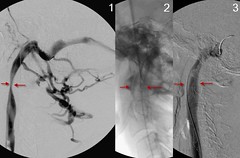
Here is an example of a narrowed J3 associated with J1 segment valve stenosis. Treatment of valve stenosis only withimporovements

Here is an example of a compressed J3 stent
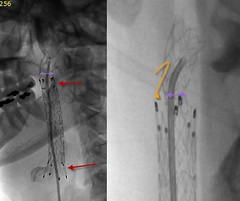
Here is an example of a compressed J3 stent (placed by another IR) with secondary intimal hyperplasia
Here is a J3 stent with in-stent stenosis
My takehome messages to you are:
1. J-3 stenosis are rarely isolated. They are usually associated with valvular stenosis
2. treatment of valvular stenosis may make improvements. This is especially tru if the IJV on the other side is also highly stenotic
3. J3 segment lesions frequently require stents, which have some complications
4. Make sure that you get a very thorough venogram with IVUS to best evaluate what you have and to optimize your treatment plan.
Hope that this helps you
DrSclafani