each balloon inflation leads to stagnation of blood above the balloon. I deflate the balloon periodically to wash this blood away and avoid clotting. however the hypoplastic vein carries little blood so clot is possible.Cece wrote:Was it unusual then for the clots to form the way they did and the thrombectomy catheter to be needed? Why would a hypoplastic vein have more clotting that quickly, if indeed this is unusual?drsclafani wrote:This patient was anticoagulated before getting on the procedural table.
DrSclafani answers some questions
-
drsclafani

- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
-
Algis

- Family Elder
- Posts: 829
- Joined: Sat Nov 21, 2009 3:00 pm
- Location: XinYi District, Taipei City, , Taiwan
Why don't they make hollow balloons? Inflating tube?each balloon inflation leads to stagnation of blood above the balloon. I deflate the balloon periodically to wash this blood away and avoid clotting.
*** EDIT ***
This Question has been replied by Doctor Sclafani already; but due to technical mayhem it was deleted .
Answer was (globally) - Cost, efficacy and practical.
Last edited by Algis on Fri Dec 17, 2010 2:03 am, edited 1 time in total.
-
ErikaSlovakia
- Family Elder
- Posts: 1125
- Joined: Wed Jul 29, 2009 2:00 pm
- Location: Slovakia, Europe
- Contact:
Endothelin 1 was discussed in this thread:Talisker wrote:Is there a method of detecting apoptosis of Endothelial cells or Astrocytes from a blood sample. If so has any studies been done on CCSVI patients?
http://www.thisisms.com/ftopict-14320-endothelin.html
Maybe you can find something there.
Erika
Aug. 7, 09 Doppler Ultras. in Poland, left Jugul. valve problem, RRMS since 1996, now SPMS,
- Nov.3,09: one stent in the left jug. vein in Katowice, Poland, LDN, never on DMDs
- Jan. 19, 11: control venography in Katowice - negative but I feel worse
- Nov.3,09: one stent in the left jug. vein in Katowice, Poland, LDN, never on DMDs
- Jan. 19, 11: control venography in Katowice - negative but I feel worse
Erika posted a great link. 
There is also the hemosiderin urine test, previously investigated by Dr. Zamboni in CVI, I asked about it once here and got a "we shall see":
http://www.thisisms.com/ftopicp-138009.html#138009
There is also the hemosiderin urine test, previously investigated by Dr. Zamboni in CVI, I asked about it once here and got a "we shall see":
http://www.thisisms.com/ftopicp-138009.html#138009
That makes sense, thanks for explaining. We talked about clotting during the procedure once in regards to duration of ballooning. It also fits with your first patient, you've said that it was a "very diseased vein," if that played a role in the overnight clotting. I've heard of another respected doctor who chooses his anticoagulation scheme (from nothing to aspirin to coumadin to heparin or maybe heparin-like) based on the flow results the day after the procedure. If good flow helps prevent clotting, I can see the reasoning there, but I don't like the assumption that what is present the day after the procedure will stay that way even in the short term. Can't wait for progress to be made in terms of standardization. These voyages of discovery are a little shaky.drsclafani wrote:each balloon inflation leads to stagnation of blood above the balloon. I deflate the balloon periodically to wash this blood away and avoid clotting. however the hypoplastic vein carries little blood so clot is possible.
Neck pain
Dr. Sclafani,
Thank you for all the work you have put into answering our questions.
I just wanted to ask one thing.
I had balloon angioplasty of my left jugular vein in July 2010. I still have pain in that area on and off, every few days, particularly when I'm tired. I'm considering going back for a checkup and possible further angioplasty, but I dont want to risk it if there is a problem with my vein - if it is damaged etc.
Would you have any thoughts on what the cause of this pain could be,and whether it would be safe to angioplasty an area that is in occasional pain?
I also have occasional pain behind my left ear. I'm not sure if this is related or relevant.
Thank you so much.
Thank you for all the work you have put into answering our questions.
I just wanted to ask one thing.
I had balloon angioplasty of my left jugular vein in July 2010. I still have pain in that area on and off, every few days, particularly when I'm tired. I'm considering going back for a checkup and possible further angioplasty, but I dont want to risk it if there is a problem with my vein - if it is damaged etc.
Would you have any thoughts on what the cause of this pain could be,and whether it would be safe to angioplasty an area that is in occasional pain?
I also have occasional pain behind my left ear. I'm not sure if this is related or relevant.
Thank you so much.
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: Neck pain
i would have thought that you would be going back soon for your second or third ultrasound by now.cara28 wrote:Dr. Sclafani,
Thank you for all the work you have put into answering our questions.
I just wanted to ask one thing.
I had balloon angioplasty of my left jugular vein in July 2010. I still have pain in that area on and off, every few days, particularly when I'm tired. I'm considering going back for a checkup and possible further angioplasty, but I dont want to risk it if there is a problem with my vein - if it is damaged etc.
Would you have any thoughts on what the cause of this pain could be,and whether it would be safe to angioplasty an area that is in occasional pain?
I also have occasional pain behind my left ear. I'm not sure if this is related or relevant.
Thank you so much.
seems like a long time to have pain from angioplasty. Need more information about balloon size, inflation pressure, etc.
Get an ultrasound
It is often said that two or more blockages of the main draining pathways of brain and spinal cord are necessary for MS/CCSVI symptoms to emerge.
In case repeated angiographies fail to recognize more than one, would you suggest preventative ballooning of usually affected areas?
Extending this, under what circumstances would you regard only one blockage as sufficient enough?
In case repeated angiographies fail to recognize more than one, would you suggest preventative ballooning of usually affected areas?
Extending this, under what circumstances would you regard only one blockage as sufficient enough?
mo_en, one of Dr. Sclafani's patients had only a single jugular treated but has happily had good results!
here is Malden asking if it takes two obstructions and drsclafani responding that it takes two findings on Doppler ultrasound:
http://www.thisisms.com/ftopicp-136764.html#136764
here is Malden asking if it takes two obstructions and drsclafani responding that it takes two findings on Doppler ultrasound:
http://www.thisisms.com/ftopicp-136764.html#136764
-
LadyGazelle

- Family Member
- Posts: 48
- Joined: Sat Jul 03, 2010 2:00 pm
- Location: Rochester, New York
- Contact:
Follow up CCSVI report..
I have typed up the full report at the bottom of my blog that explains all that was done at my CCSVI treatment in Albany. I did the pre-lib video, but this will explain why I didn't get any good results. They were temporary for a week, but since then after reading my report, it looks like my vertebra is squeezing my LIJV.
I wrote to the Upright Doc here, and he said it sounds like I have spondylosis - and I also have degenerative disc disease after a whiplash. So, if you want good blood flow - be sure your bones are in alignment.
Go to www.ccsvi-ms.blogspot.com to learn more.
I am going to see a NUCCA chiropractor if she takes Medicaid. There are only 21 board certified chiropractors that are specially trained in upper cervical chiropractic, and one is 10 minutes from my home! I hope she can help open my veins. Or at least fix my spine so it can be ballooned open!
Even though I don't see improvement now, it doesn't mean it can't happen. I will keep that hope alive, and this information helps you.
Lady Gazelle
I wrote to the Upright Doc here, and he said it sounds like I have spondylosis - and I also have degenerative disc disease after a whiplash. So, if you want good blood flow - be sure your bones are in alignment.
Go to www.ccsvi-ms.blogspot.com to learn more.
I am going to see a NUCCA chiropractor if she takes Medicaid. There are only 21 board certified chiropractors that are specially trained in upper cervical chiropractic, and one is 10 minutes from my home! I hope she can help open my veins. Or at least fix my spine so it can be ballooned open!
Even though I don't see improvement now, it doesn't mean it can't happen. I will keep that hope alive, and this information helps you.
Lady Gazelle

venous calcium deposits
Hi Dr. Sclafani,
A ThisIsMS member reported in another thread that their doctors had found a calcium deposit in their azygos vein near a valve. It was inferred that this deposit might be interfering with the normal function of the valve. The vein was ballooned, but this person only had temporary benefit.
In light of the above discussion, it would be great if you could comment on the potential benefit of taking vitamin K2 to help remove calcium deposits from blood vessels. Are calcium deposits commonly seen in CCSVI veins? If so, vitamin K2 could be of benefit (or perhaps at least in the above instance).
Thanks, NHE
A ThisIsMS member reported in another thread that their doctors had found a calcium deposit in their azygos vein near a valve. It was inferred that this deposit might be interfering with the normal function of the valve. The vein was ballooned, but this person only had temporary benefit.
In light of the above discussion, it would be great if you could comment on the potential benefit of taking vitamin K2 to help remove calcium deposits from blood vessels. Are calcium deposits commonly seen in CCSVI veins? If so, vitamin K2 could be of benefit (or perhaps at least in the above instance).
Thanks, NHE
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
True enough.mo_en wrote:It is often said that two or more blockages of the main draining pathways of brain and spinal cord are necessary for MS/CCSVI symptoms to emerge.
In case repeated angiographies fail to recognize more than one, would you suggest preventative ballooning of usually affected areas?
Extending this, under what circumstances would you regard only one blockage as sufficient enough?
but which two vessels can be significant?
This case describes a 40 year old man with chief complaints of cognitive dysfunction, severe fatigue, periodic migraine headaches, temperature intolerance, spasticity and urinary frequency.
Doppler and Bmode ultrasound of the neck and transcranial power doppler of the deep cerebral veins revealed two Zamboni criteria for CCSVI.
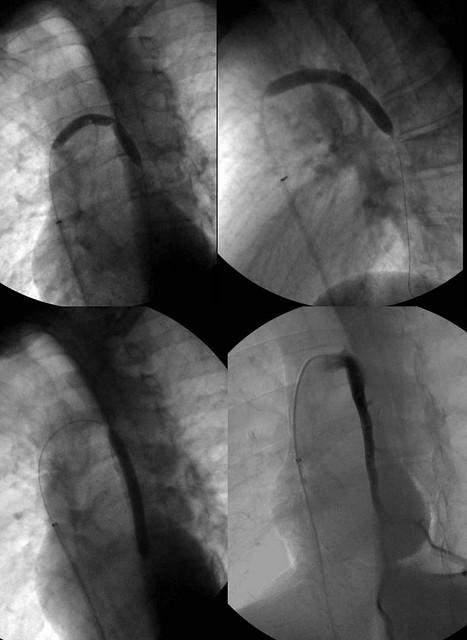
Venography was performed to assess the cause of the CCSVI.
Right and Left internal jugular venography was performed. While there was questionable minimal narrowing of the left jugular confluens but flow was brisk and no stasis or reflux was visible. The right internal jugular vein looked normal.

Azygos venography showed a thickened valvular area (red arrow), outflow obstruction (green arrow) and reflux in the descending portion of the vein (orange curved arrows)

Angioplasty was performed of the descending azygos vein and the azygos arch. The final image on the right bottom shows reduction in collaterals and better flow.
So how can this be that one outlet obstruction can cause such symptoms?
imaging of the vertebral veins illustrates that an outlet of a second system IS present. Both vertebral veins are incomplete.

So as we explore, we find that the permutations of vascular anomalies are many. While we have simple answers to some of these anomalies and are moving toward refined methods of treatment, for others we remain novice. How to deal with vertebral vein problems is more complex and will await further thought.
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Re: venous calcium deposits
i am skeptical of this diagnosis. it is more likely contrast media trapped under a malformed valve.NHE wrote:Hi Dr. Sclafani,
A ThisIsMS member reported in another thread that their doctors had found a calcium deposit in their azygos vein near a valve. It was inferred that this deposit might be interfering with the normal function of the valve. The vein was ballooned, but this person only had temporary benefit.
In light of the above discussion, it would be great if you could comment on the potential benefit of taking vitamin K2 to help remove calcium deposits from blood vessels. Are calcium deposits commonly seen in CCSVI veins? If so, vitamin K2 could be of benefit (or perhaps at least in the above instance).
Thanks, NHE
i would not treat until this is cleared up
If you'd ended this here to stimulate discussion, I would not have guessed the verts. (I would have guessed that it was because of the importance of the azygous, draining the spine which cannot reroute as easily as the brain, & Dr. Zamboni's 'pattern D' with just azygous involvement.)drsclafani wrote:So how can this be that one outlet obstruction can cause such symptoms?
Does incomplete mean that it's partial agenesis of the vertebral veins? I would think a valve issue in the verts might eventually be treatable (you mentioned back in June that Dr. Galleotti had tried treating the verts with negligible or mixed results?) but agenesis would be really tricky. But if it takes two obstructions to cause problems, the clearing of one of the obstructions might yet be enough to relieve the problems.imaging of the vertebral veins illustrates that an outlet of a second system IS present. Both vertebral veins are incomplete.
Thanks for sharing these latest images and case study.

Re: Follow up CCSVI report..
I have a problem with the concept of your vertebra squeezing your LIJV.LadyGazelle wrote:I have typed up the full report at the bottom of my blog that explains all that was done at my CCSVI treatment in Albany. I did the pre-lib video, but this will explain why I didn't get any good results. They were temporary for a week, but since then after reading my report, it looks like my vertebra is squeezing my LIJV.
I wrote to the Upright Doc here, and he said it sounds like I have spondylosis - and I also have degenerative disc disease after a whiplash. So, if you want good blood flow - be sure your bones are in alignment.
Go to www.ccsvi-ms.blogspot.com to learn more.
I am going to see a NUCCA chiropractor if she takes Medicaid. There are only 21 board certified chiropractors that are specially trained in upper cervical chiropractic, and one is 10 minutes from my home! I hope she can help open my veins. Or at least fix my spine so it can be ballooned open!
Even though I don't see improvement now, it doesn't mean it can't happen. I will keep that hope alive, and this information helps you.
Lady Gazelle
As you know veins can easily go around any fixed structures. To affect a vein you need to squeeze it between 2 opposing structures.
This is not just semantic but will let you and all of us, understand better what is going on. My guess, after reading Dr. Noda article on CTOS is that it is one of the Scalene muscles. The implication is that dilation by balloon angioplasty would not work because the muscle would still squeeze the LIJV against your vertebra. I do not know about chiropractic maneuver. It will depend on how much the doctor will be able to move your vertebra.
In the future I envision using external stents to prevent extrinsic compression of the Jugular vein. I know Dr.Noda was releasing the scalene muscle to prevent compression.
The same concept goes for people claiming they have the carotid bulb indenting the Jugular vein.
Your problem is that Gazelle have a long neck prone to these misalignment problems. If you were an Hippopotamus with a short neck, you might be just fine even though "lady Hippopotamus" doesn't have the same ring as "lady Gazelle"
Good luck on your new treatment.
Everybody here brings happiness, somebody by coming,others by leaving. PPMS since 2000<br />