Dr. Sclafani,
Concerning left IJV only.
What if little to no flow in the left IJV is noted via MRV (left side drainage primarily a facial vein & vertebral plexus), the doppler shows a septum and stenosis in the left IJV....what are the possible treatment scenarios in this case?
DrSclafani answers some questions
With periodic dilation, if you could possibly continue to increase the size of the vein, do you have a size in mind as a goal? With this vein, did you get close to that size?drsclafani wrote:not a bad beginning but reconstruction may take more than one treatment. So we come to another question, should periodic dilatation be performed or is one treatment sufficient until restenosis. This is unanswered. at the momen
Is there any rationale behind the 2-3 week interval in arteriovenous fistula maturation? Why not shorter (1 week?) or longer (2 months? 6 months?). If it could be done at a different interval, it might be more of an option for some of your travelling patients, if the benefit seemed to be there.
Fantastic images. What an opportunity for us, and any lurking MDs, to learn and see.
-
drsclafani

- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
all good possibilities.mo_en wrote:A very enlightening post it was about treating hypoplasia.
And now a riddle: 25 year old MS patient has effectively had her azygos, right and left jugular veins treated in three successive angioplasties. Her symptoms deteriorate. A fourth angiogram shows perfect flow to all three veins. Cortisone therapy has no effect. An MRI of head & neck shows no new or enhancing lesions. Her symptoms deteriorate again. Vertigo, numbness and balance issues.
What seems to be the problem? An unresolved stenosis? Venous back-jets through the valveless jugulars? Increased flow in vertebral plexus and subsequent load on spine lesions? Or just a roller coaster improvement?
as always the next step is a doppler.
tell me, was ultrasound done before each angioplasty
i have recently had sent to me some images that i was told looked pretty normal. however my read was stenosis bilaterally in the jugulars and inconclusive imaging in the azygos.
unfortunately the person who sent them to me did not tell me history, just sent the images
so it is hard to answer from what you describe.
so first off the ultrasound suite for a check of the hemodynamimcs
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
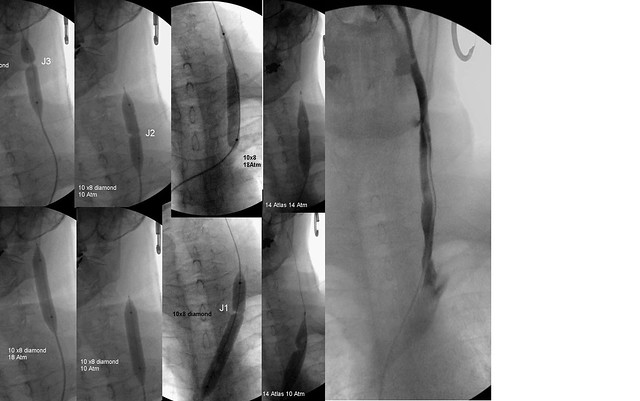
nunzioNunzio wrote:Hi Dr. Sclafani,drsclafani wrote: So a hypoplasia correction procedure was performed in one treatment.
First 10 millimeter 8 cm long balloons were used to dilate the J3, J2 and J1 regions. 10 Atmospheres were sufficient to overcome all stenoses except annular stenosis at the confluens. Finally 14 mm balloons were used to overcome stenotic areas in J1.
the final image on the right shows the ultimate appearance of the veins. No collaterals were noted..
one would anticipate that this patient has notseen her last day in this department.
not a bad beginning but reconstruction may take more than one treatment. So we come to another question, should periodic dilatation be performed or is one treatment sufficient until restenosis. This is unanswered. at the momen
I am very impressed by the fact you were able to dilate a totally hypoplastic vein to a 14 mm. diameter in just one session. As you probably remember this is my case too so I am particularly interested in this subject.
My concern is that it might be difficult to dilate the IJV near the bony ostium because of the fixed stricture that might not allow the balloon to properly expand.
The other problem is that if there is poor flow from the sigmoid/transverse sinus then there is higher chance of thrombosis due to the low velocity of the blood traveling through the newly dilated vein.
Because it would be nice to have higher flow also to prevent re-narrowing,
I wonder if you have some insight on the possibility of dilating the sinuses.
This is a scary thought for me because of what is next to the sinus.
Thanks again and Buon Natale.
i am in total agreement with you on all considerations. Firstly the high pressure balloons have a long nose and it is pretty difficult to get them to go through the jugular foramen. on the other hand, the jugular vein is always smaller at the skull base than it is near the confluens.
Secondly i am terrified of dilating this segment because of the risk benefit ratio is not so obviously in favor of taking the risk.
thirdly, the dural sinus anatomy ifs highly variable and i am not sure what exactly is pathological.
my group of neuroradiologists at the hospital will soon begin a retrospective analysis of the deep cerebral veins on cta performed for stroke in non MS stroke patients. more than jugular vein anatomay, dural sinus anatomy is quite variable.
if such a procedure were justified, i would hand off to my neuro-interventional radiologist to take care of IN THE HOSPITAL with neurosurgical backup....call me chicken
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
put up catheter in, inflate balloonpairOdime wrote:Dr. Sclafani,
Concerning left IJV only.
What if little to no flow in the left IJV is noted via MRV (left side drainage primarily a facial vein & vertebral plexus), the doppler shows a septum and stenosis in the left IJV....what are the possible treatment scenarios in this case?
seriously, one cannot make a strategy based upon your description. firstly mrv is not my cup of tea
secondly mostly we see hemdynamics on ultrasound rather than the anatomical derangements that i treat.
i would say that venography is first, then IVUS, then treatment depending on what these two tests show
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
female 18Cece wrote:With periodic dilation, if you could possibly continue to increase the size of the vein, do you have a size in mind as a goal? With this vein, did you get close to that size?drsclafani wrote:not a bad beginning but reconstruction may take more than one treatment. So we come to another question, should periodic dilatation be performed or is one treatment sufficient until restenosis. This is unanswered. at the momen
male 20
give or take a couple of millimeters.
recuperation, elastic recoil, healing of intima?Is there any rationale behind the 2-3 week interval in arteriovenous fistula maturation? Why not shorter (1 week?) or longer (2 months? 6 months?). If it could be done at a different interval, it might be more of an option for some of your travelling patients, if the benefit seemed to be there.
i dont know, i will ask my colleagues
i remember my first case. i had seen about six venographic images so it was quite challenging to know what was abnormal, how significant narrowings could be, etc.Fantastic images. What an opportunity for us, and any lurking MDs, to learn and see.
to any lurking physicians out there, welcome to the lecture hall
-
drsclafani
- Family Elder
- Posts: 3182
- Joined: Fri Mar 12, 2010 3:00 pm
- Location: Brooklyn, New York
- Contact:
Now that is a picture that might have a story behind it!
Unless that is your lawn...I can't quite make out the bus stop....
I checked google scholar, I didn't find anything easily.
In thinking it over, if this is usually a time-pressing situation where the patients need to get onto dialysis (if it's the AVF maturation), that might be why they wouldn't do the procedures further apart in time (but perhaps it's perfectly fine to do so, in CCSVI).
Unless that is your lawn...I can't quite make out the bus stop....
I liked this response.drsclafani wrote:recuperation, elastic recoil, healing of intima?Is there any rationale behind the 2-3 week interval in arteriovenous fistula maturation? Why not shorter (1 week?) or longer (2 months? 6 months?). If it could be done at a different interval, it might be more of an option for some of your travelling patients, if the benefit seemed to be there.
i dont know, i will ask my colleagues
I checked google scholar, I didn't find anything easily.
In thinking it over, if this is usually a time-pressing situation where the patients need to get onto dialysis (if it's the AVF maturation), that might be why they wouldn't do the procedures further apart in time (but perhaps it's perfectly fine to do so, in CCSVI).
The first ultrasound revealed abnormal flow in both jugulars, the following angiogram only an azygos occlusion; fixed. The second ultrasound found a stenosis on the left. Confirmed by the angiogram; fixed. Then the right, the same way. The fourth ultrasound was ok, the angiogram as well.tell me, was ultrasound done before each angioplasty
To be noted, the deep cerebral veins were checked only on first ultrasound.
-
newlywed4ever
- Family Elder
- Posts: 255
- Joined: Thu Apr 17, 2008 2:00 pm
- Location: Michigan
- Contact:

I would advise her to repeat the procedure. The risks of angioplasty are comparatively low and you already know that the benefits could be great. I'm no doctor so perhaps my advice is not so valuable but it sounds as though it has to be done.sara-sama wrote:hi ..
I'm happy to join you and I hope to find Benefit with you ..
My sister have Als .. diagnosed 18 months ago
she did the doppler ultrasound .. Then Found stenosis 90% on both sides of the neck ..
When she Got"The Liberation Procedure" By the balloon Since 6 months ago
her face color became Normal .. movement of her hands more flexible .. Swallowing Better .. Speech is becoming more clarity ..and no depression
But all of this improvement was for only one Month and returned deteriorate ..
She lost the ability to movement, speech and swallowing within 18 months .. Now she wants to travel to angioplasty procedure again ,Do you support that.. Do you think that the health status allow it ..What is your advice?
It makes me very glad to hear that there were benefits in the past and that there is a good chance that the loss of benefit, probably due to restenosis, will be reversed. With ALS. Incredible. Yes, I am very pleased for your sister and I hope that she gets the benefits back.
L wrote:I would advise her to repeat the procedure. The risks of angioplasty are comparatively low and you already know that the benefits could be great. I'm no doctor so perhaps my advice is not so valuable but it sounds as though it has to be done.sara-sama wrote:hi ..
I'm happy to join you and I hope to find Benefit with you ..
My sister have Als .. diagnosed 18 months ago
she did the doppler ultrasound .. Then Found stenosis 90% on both sides of the neck ..
When she Got"The Liberation Procedure" By the balloon Since 6 months ago
her face color became Normal .. movement of her hands more flexible .. Swallowing Better .. Speech is becoming more clarity ..and no depression
But all of this improvement was for only one Month and returned deteriorate ..
She lost the ability to movement, speech and swallowing within 18 months .. Now she wants to travel to angioplasty procedure again ,Do you support that.. Do you think that the health status allow it ..What is your advice?
It makes me very glad to hear that there were benefits in the past and that there is a good chance that the loss of benefit, probably due to restenosis, will be reversed. With ALS. Incredible. Yes, I am very pleased for your sister and I hope that she gets the benefits back.
Thanks a lot "L"
I hope that my sister get another chance, the results of previous experience was fantastic, especially swallowing ..
sara-sama, I agree with L too. If we look at CCSVI as a separate condition from MS or from ALS, it warrants treatment in its own right IMO. Your sister has been diagnosed with two disorders.
My only caution is that for whatever reason sometimes people are not getting the same results after their second procedure that they experienced after their first. I don't understand why that would be. And sometimes, they get the exact same results or better. Your sister has all of our best wishes, I hope you will keep us updated.
My only caution is that for whatever reason sometimes people are not getting the same results after their second procedure that they experienced after their first. I don't understand why that would be. And sometimes, they get the exact same results or better. Your sister has all of our best wishes, I hope you will keep us updated.
Thanks Cece,Cece wrote:sara-sama, I agree with L too. If we look at CCSVI as a separate condition from MS or from ALS, it warrants treatment in its own right IMO. Your sister has been diagnosed with two disorders.
My only caution is that for whatever reason sometimes people are not getting the same results after their second procedure that they experienced after their first. I don't understand why that would be. And sometimes, they get the exact same results or better. Your sister has all of our best wishes, I hope you will keep us updated.
I hope she can travel and repeat the catheter without risk ..